

Epidemiology and outcomes of elderly patients requiring renal replacement therapy in the intensive care unit: an observational study
- PMID: 33740897
- PMCID: PMC7980322
- DOI: 10.1186/s12882-021-02302-4
Epidemiology and outcomes of elderly patients requiring renal replacement therapy in the intensive care unit: an observational study
Abstract
Background: Renal replacement therapy (RRT) in critically ill patients is associated with high morbidity and mortality. The appropriateness of RRT initiation is sometimes questioned in elderly patients. Therefore, we sought to evaluate the long-term mortality, dialysis dependence and quality of life (QOL) of elderly patients who survived critical illness requiring RRT.
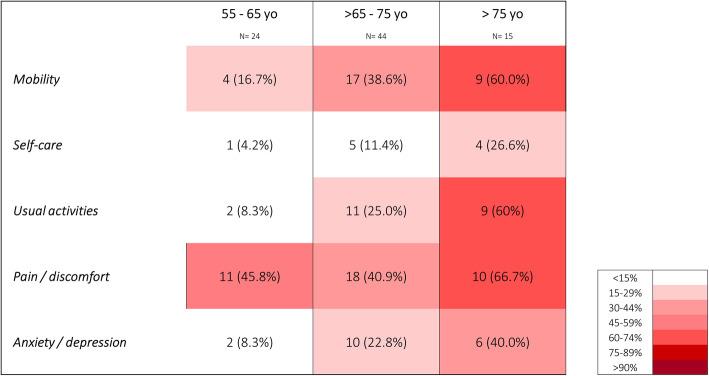
Methods: This is a monocentric observational study including all patients > 55 yo who received RRT for acute kidney injury in our intensive care unit (ICU) between January 2015 and April 2018. At the time of the study (May 2019), we assessed if they were still alive by cross referencing our hospital database and the Swiss national death registry. We sent survivors written information and, subsequently, contacted them over the phone. We obtained their consent for participation, asked about their dialytic status and performed an EQ-5D survey with visual analog scale (VAS). Results were stratified according to their age at the time of ICU admission (G1: "55-65 yo"; G2: "> 65-75 yo" and G3: "> 75 yo"). QOL in G3 patients were compared to G1 and G2 and to predicted values.
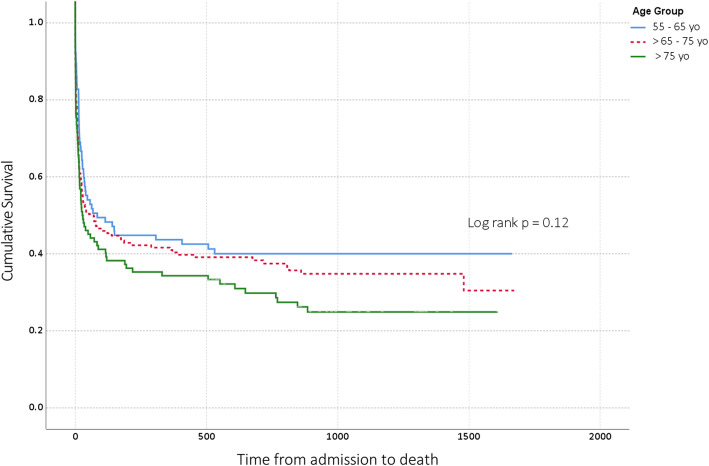
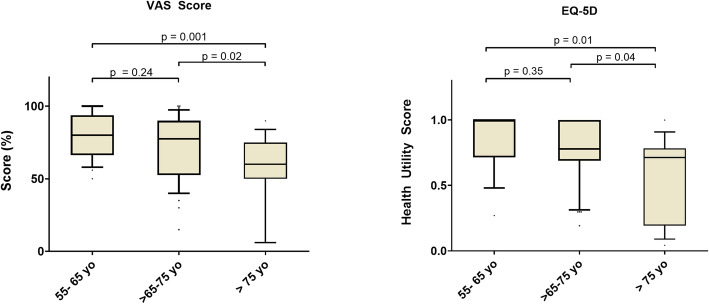
Results: Among the 352 eligible patients, 171 died during the index hospital admission. After a median follow-up time of 32.7 months (IQR 19.8), a further 62 had died (median time to death for ICU survivors 5.0 (IQR 15.0) months. Hence, 119 (33.6%) patients were still alive at the time of the study. We successfully contacted 96 (80.7%) of them and 83 (69.7%) were included in the study (G1: 24, G2: 44 and G3: 15). Only 6 (7.2%) were RRT dependent. Patients in G3 had lower EQ-5D and VAS scores than those in G1 and G2 (p < 0.01). These scores were also significantly lower than predicted values (p < 0.05).
Conclusions: RRT patients have a very high in-hospital and post discharge mortality. Among survivors, RRT dependency was low. Irrespective of baseline values, patients > 75 yo who survived ICU had a lower QOL than younger patients. It was lower than predicted according to age and sex. The appropriateness of RRT initiation in elderly patients should be discussed according to their pre-existing QOL and frailty.
Keywords: Acute kidney injury (AKI); Elderly; Mortality; Quality of life (QOL); Renal replacement therapy (RRT).
Conflict of interest statement
CS, MA, NB and EP stated that they had no conflicts of interest to declare.
AGS has received a grant from the Leenaards foundation, speaker honoraria from Fresenius Medical Care and consulting honoraria from B Braun Melsungen AG.
Figures
References
-
- de Rooij SE, Govers AC, Korevaar JC, Giesbers AW, Levi M, de Jonge E. Cognitive, functional, and quality-of-life outcomes of patients aged 80 and older who survived at least 1 year after planned or unplanned surgery or medical intensive care treatment. J Am Geriatr Soc. 2008;56(5):816–822. doi: 10.1111/j.1532-5415.2008.01671.x. - DOI - PubMed
-
- Le Borgne P, Maestraggi Q, Couraud S, Lefebvre F, Herbrecht JE, Boivin A, Michard B, Castelain V, Kaltenbach G, Bilbault P, et al. Critically ill elderly patients (>/= 90 years): clinical characteristics, outcome and financial implications. PLoS One. 2018;13(6):e0198360. doi: 10.1371/journal.pone.0198360. - DOI - PMC - PubMed
-
- Gallagher M, Cass A, Bellomo R, Finfer S, Gattas D, Lee J, Lo S, McGuinness S, Myburgh J, Parke R, Rajbhandari D, for the POST-RENAL Study Investigators and the ANZICS Clinical Trials Group Long-term survival and Dialysis dependency following acute kidney injury in intensive care: extended follow-up of a randomized controlled trial. PLoS Med. 2014;11(2):e1001601. doi: 10.1371/journal.pmed.1001601. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
