

Laparoscopic proximal gastrectomy with double-tract reconstruction for upper third gastric cancer
- PMID: 33740923
- PMCID: PMC7977324
- DOI: 10.1186/s12893-021-01153-y
Laparoscopic proximal gastrectomy with double-tract reconstruction for upper third gastric cancer
Abstract
Background: Proximal gastrectomy with double-tract reconstruction (DTR) has been used for upper third gastric cancer as a function-preserving procedure. However, the safety and feasibility of laparoscopic proximal gastrectomy (LPG) with DTR remain uncertain. This study compared open proximal gastrectomy (OPG) with DTR and LPG with DTR for proximal gastric cancer.
Methods: Sixty-four patients who had undergone OPG with DTR and forty-six patients who had undergone LPG with DTR were enrolled in this case-control study. The clinical characteristics, surgical outcomes and postoperative nutrition index were analysed retrospectively.
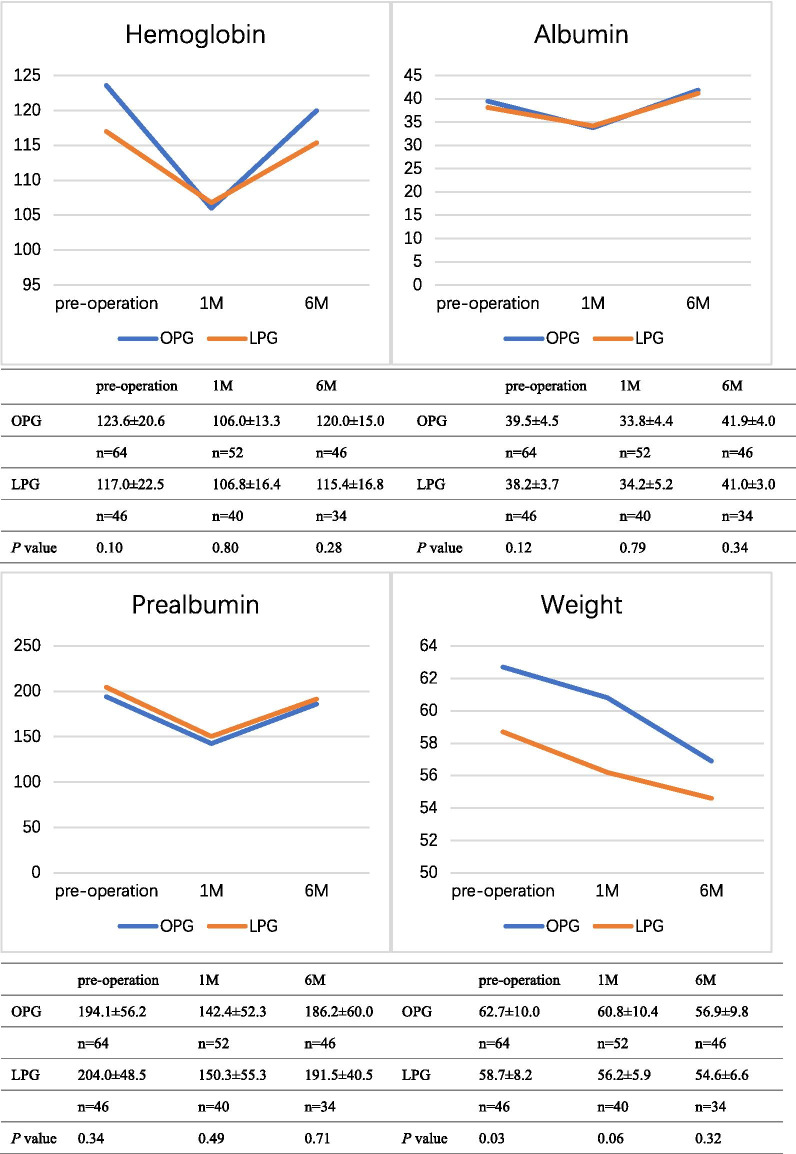
Results: The operation time was significantly longer in the LGP group than in the OPG group (258.3 min vs 205.8 min; p = 0.00). However, the time to first flatus and postoperative hospital stay were shorter in the LPG group [4.0 days vs 3.5 days (p = 0.00) and 10.6 days vs 9.2 days (p = 0.001), respectively]. No significant difference was found between the two groups in the number of retrieved lymph nodes, complications or reflux oesophagitis. The nutrition status was assessed using the haemoglobin, albumin, prealbumin and weight levels from pre-operation to six months after surgery. No significant difference was found between the groups.
Conclusion: LPG with DTR can be safely performed for proximal gastric cancer patients by experienced surgeons.
Keywords: Double-tract reconstruction; Feasibility; Gastric cancer; Laparoscopy proximal gastrectomy; Open proximal gastrectomy; Safety.
Conflict of interest statement
All authors declare they have no competing interests.
Figures
Similar articles
-
[Efficacy of laparoscopic proximal gastrectomy with double-tract reconstruction versus laparoscopic total gastrectomy with Roux-en-Y reconstruction for early upper gastric cancer].Zhonghua Wei Chang Wai Ke Za Zhi. 2022 May 25;25(5):412-420. doi: 10.3760/cma.j.cn441530-20211118-00466. Zhonghua Wei Chang Wai Ke Za Zhi. 2022. PMID: 35599396 Chinese.
-
Short-term outcomes and quality of life of esophagogastrostomy versus the double-tract reconstruction after laparoscopic proximal gastrectomy.BMC Cancer. 2024 Oct 28;24(1):1324. doi: 10.1186/s12885-024-13095-8. BMC Cancer. 2024. PMID: 39468480 Free PMC article.
-
Laparoscopic proximal gastrectomy with double tract reconstruction is superior to laparoscopic total gastrectomy for proximal early gastric cancer.Surg Endosc. 2017 Oct;31(10):3961-3969. doi: 10.1007/s00464-017-5429-9. Epub 2017 Mar 24. Surg Endosc. 2017. PMID: 28342130
-
Proximal Gastrectomy for Gastric Cancer.J Gastric Cancer. 2015 Jun;15(2):77-86. doi: 10.5230/jgc.2015.15.2.77. Epub 2015 Jun 30. J Gastric Cancer. 2015. PMID: 26161281 Free PMC article. Review.
-
Laparoscopic proximal gastrectomy for early gastric cancer.Surg Today. 2017 May;47(5):538-547. doi: 10.1007/s00595-016-1401-x. Epub 2016 Aug 22. Surg Today. 2017. PMID: 27549773 Review.
Cited by
-
Comparison of clinical efficacy between π-shaped esophagojejunostomy and overlap method in treating upper gastric cancer with double-tract reconstruction in proximal gastrectomy under total laparoscopy.World J Surg Oncol. 2025 Apr 7;23(1):120. doi: 10.1186/s12957-025-03768-4. World J Surg Oncol. 2025. PMID: 40189553 Free PMC article.
-
The Safety and Anti-Reflex Effect of Robotic Double-Tract Reconstruction After Proximal Gastrectomy for Gastric Cancer.Asian J Endosc Surg. 2025 Jan-Dec;18(1):e70001. doi: 10.1111/ases.70001. Asian J Endosc Surg. 2025. PMID: 39675837 Free PMC article.
-
The Short-Term and Long-Term Outcomes of Laparoscopy-Assisted Proximal Gastrectomy with Double-Tract Reconstruction versus Laparoscopy-Assisted Total Gastrectomy with Roux-en-Y Reconstruction for Adenocarcinoma of the Esophagogastric Junction: A Multicenter Study Based on Propensity Score Matching Analysis.Gastroenterol Res Pract. 2024 May 27;2024:5517459. doi: 10.1155/2024/5517459. eCollection 2024. Gastroenterol Res Pract. 2024. PMID: 38882392 Free PMC article.
-
The clinical outcomes of laparoscopic proximal gastrectomy with double-tract reconstruction versus tube-like stomach reconstruction in patients with adenocarcinoma of the esophagogastric junction based on propensity score-matching: a multicenter cohort study.Front Oncol. 2023 Jun 2;13:1137836. doi: 10.3389/fonc.2023.1137836. eCollection 2023. Front Oncol. 2023. PMID: 37333809 Free PMC article.
-
Laparoscopic Function-Preserving Gastrectomy for Proximal Gastric Cancer or Esophagogastric Junction Cancer: A Narrative Review.Cancers (Basel). 2023 Jan 3;15(1):311. doi: 10.3390/cancers15010311. Cancers (Basel). 2023. PMID: 36612308 Free PMC article. Review.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
