

Association between Medicare's Hospital Readmission Reduction Program and readmission rates across hospitals by medicare bed share
- PMID: 33740969
- PMCID: PMC7980319
- DOI: 10.1186/s12913-021-06253-2
Association between Medicare's Hospital Readmission Reduction Program and readmission rates across hospitals by medicare bed share
Abstract
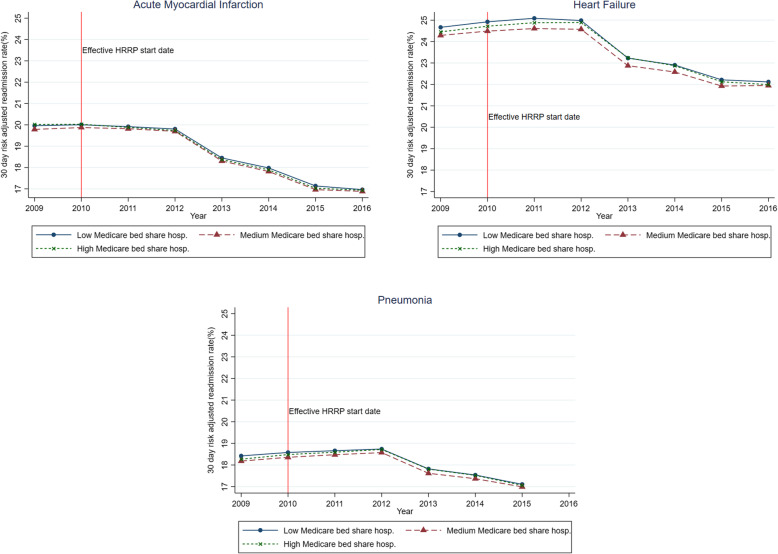
Background: Medicare's Hospital Readmissions Reduction Program (HRRP), implemented beginning in 2013, seeks to incentivize Inpatient Prospective Payment System (IPPS) hospitals to reduce 30-day readmissions for selected inpatient cohorts including acute myocardial infarction, heart failure, and pneumonia. Performance-based penalties, which take the form of a percentage reduction in Medicare reimbursement for all inpatient care services, have a risk of unintended financial burden on hospitals that care for a larger proportion of Medicare patients. To examine the role of this unintended risk on 30-day readmissions, we estimated the association between the extent of their Medicare share of total hospital bed days and changes in 30-day readmissions.
Methods: We used publicly available nationwide hospital level data for 2009-2016 from the Centers for Medicare and Medicaid Services (CMS) Hospital Compare program, CMS Final Impact Rule, and the American Hospital Association Annual Survey. Using a quasi-experimental difference-in-differences approach, we compared pre- vs. post-HRRP changes in 30-day readmission rate in hospitals with high and moderate Medicare share of total hospital bed days ("Medicare bed share") vs. low Medicare bed share hospitals.
Results: We grouped the 1904 study hospitals into tertiles (low, moderate and high) by Medicare bed share; the average bed share in the three tertile groups was 31.2, 47.8 and 59.9%, respectively. Compared to low Medicare bed share hospitals, high bed share hospitals were more likely to be non-profit, have smaller bed size and less likely to be a teaching hospital. High bed share hospitals were more likely to be in rural and non-large-urban areas, have fewer lower income patients and have a less complex patient case-mix profile. At baseline, the average readmissions rate in the low Medicare bed share (control) hospitals was 20.0% (AMI), 24.7% (HF) and 18.4% (pneumonia). The observed pre- to post-program change in the control hospitals was - 1.35% (AMI), - 1.02% (HF) and - 0.35% (pneumonia). Difference in differences model estimates indicated no differential change in readmissions among moderate and high Medicare bed share hospitals.
Conclusions: HRRP penalties were not associated with any change in readmissions rate. The CMS should consider alternative options - including working collaboratively with hospitals - to reduce readmissions.
Keywords: Hospital performance-based penalty; Medicare bed share; Readmissions.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Jha AK. To fix the hospital readmissions program, Prioritize What Matters. JAMA Forum. 2017. - PubMed
-
- Centers for Medicare & Medicaid Services. Hospital Readmissions Reduction Program. https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpat.... Accessed 1 July 2019.
-
- Boccuti C, Casillas G. Aiming for fewer hospital U-turns: the Medicare hospital readmission reduction program. Menlo Park, CA: The Kaiser Family Foundation; 2017.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
