

Early effects of ventilatory rescue therapies on systemic and cerebral oxygenation in mechanically ventilated COVID-19 patients with acute respiratory distress syndrome: a prospective observational study
- PMID: 33741052
- PMCID: PMC7978164
- DOI: 10.1186/s13054-021-03537-1
Early effects of ventilatory rescue therapies on systemic and cerebral oxygenation in mechanically ventilated COVID-19 patients with acute respiratory distress syndrome: a prospective observational study
Abstract
Background: In COVID-19 patients with acute respiratory distress syndrome (ARDS), the effectiveness of ventilatory rescue strategies remains uncertain, with controversial efficacy on systemic oxygenation and no data available regarding cerebral oxygenation and hemodynamics.
Methods: This is a prospective observational study conducted at San Martino Policlinico Hospital, Genoa, Italy. We included adult COVID-19 patients who underwent at least one of the following rescue therapies: recruitment maneuvers (RMs), prone positioning (PP), inhaled nitric oxide (iNO), and extracorporeal carbon dioxide (CO2) removal (ECCO2R). Arterial blood gas values (oxygen saturation [SpO2], partial pressure of oxygen [PaO2] and of carbon dioxide [PaCO2]) and cerebral oxygenation (rSO2) were analyzed before (T0) and after (T1) the use of any of the aforementioned rescue therapies. The primary aim was to assess the early effects of different ventilatory rescue therapies on systemic and cerebral oxygenation. The secondary aim was to evaluate the correlation between systemic and cerebral oxygenation in COVID-19 patients.
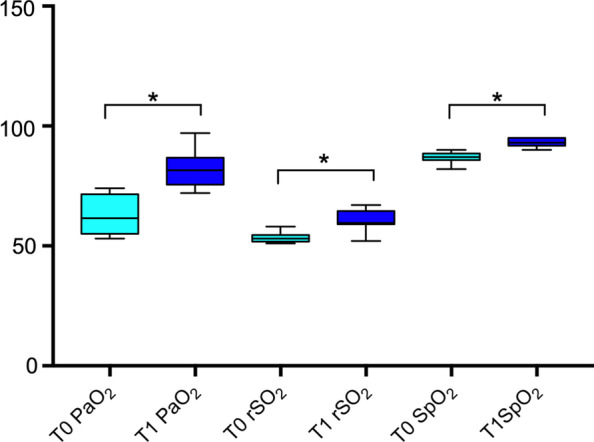
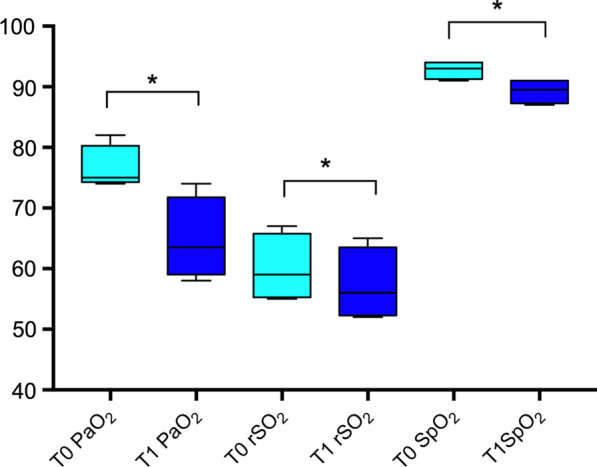
Results: Forty-five rescue therapies were performed in 22 patients. The median [interquartile range] age of the population was 62 [57-69] years, and 18/22 [82%] were male. After RMs, no significant changes were observed in systemic PaO2 and PaCO2 values, but cerebral oxygenation decreased significantly (52 [51-54]% vs. 49 [47-50]%, p < 0.001). After PP, a significant increase was observed in PaO2 (from 62 [56-71] to 82 [76-87] mmHg, p = 0.005) and rSO2 (from 53 [52-54]% to 60 [59-64]%, p = 0.005). The use of iNO increased PaO2 (from 65 [67-73] to 72 [67-73] mmHg, p = 0.015) and rSO2 (from 53 [51-56]% to 57 [55-59]%, p = 0.007). The use of ECCO2R decreased PaO2 (from 75 [75-79] to 64 [60-70] mmHg, p = 0.009), with reduction of rSO2 values (59 [56-65]% vs. 56 [53-62]%, p = 0.002). In the whole population, a significant relationship was found between SpO2 and rSO2 (R = 0.62, p < 0.001) and between PaO2 and rSO2 (R0 0.54, p < 0.001).
Conclusions: Rescue therapies exert specific pathophysiological mechanisms, resulting in different effects on systemic and cerebral oxygenation in critically ill COVID-19 patients with ARDS. Cerebral and systemic oxygenation are correlated. The choice of rescue strategy to be adopted should take into account both lung and brain needs. Registration The study protocol was approved by the ethics review board (Comitato Etico Regione Liguria, protocol n. CER Liguria: 23/2020).
Keywords: Carbon dioxide removal; Cerebral oxygenation; Coronavirus; Prone position; Recruitment maneuvers; Rescue therapies.
Conflict of interest statement
Dr. Bassetti reports personal fees and other from Angelini, personal fees and other from AstraZeneca, other from Bayer, personal fees and other from Cubist, personal fees and other from Pfizer, personal fees and other from Menarini, personal fees and other from MSD, other from Nabriva, other from Paratek, other from Roche, other from Shionogi, other from Tetraphase, other from The Medicine Company, personal fees and other from Astellas Pharma Inc., personal fees from Gilead Sciences, personal fees from Teva, personal fees from Novartis, grants from Ranbaxy, personal fees from Correvio, personal fees from Molteni, personal fees from Thermo Fisher, outside the submitted work. Dr. Giacobbe reports personal fees from Stepstone Pharma GmbH, personal fees from MSD Italia, personal fees from Correvio Italia, outside the submitted work. Dr. Matta reports personal fees from Masimo.
Figures



References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
