

A study of ethnic, gender and educational differences in attitudes toward COVID-19 vaccines in Israel - implications for vaccination implementation policies
- PMID: 33741063
- PMCID: PMC7977502
- DOI: 10.1186/s13584-021-00458-w
A study of ethnic, gender and educational differences in attitudes toward COVID-19 vaccines in Israel - implications for vaccination implementation policies
Abstract
Background: Vaccines for COVID-19 are currently available for the public in Israel. The compliance with vaccination has differed between sectors in Israel and the uptake has been substantially lower in the Arab compared with the Jewish population.
Aim: To assess ethnic and socio-demographic factors in Israel associated with attitudes towards COVID-19 vaccines prior to their introduction.
Methods: A national cross-sectional survey was carried out In Israel during October 2020 using an internet panel of around 100,000 people, supplemented by snowball sampling. A sample of 957 adults aged 30 and over were recruited of whom 606 were Jews (49% males) and 351 were Arabs (38% males).
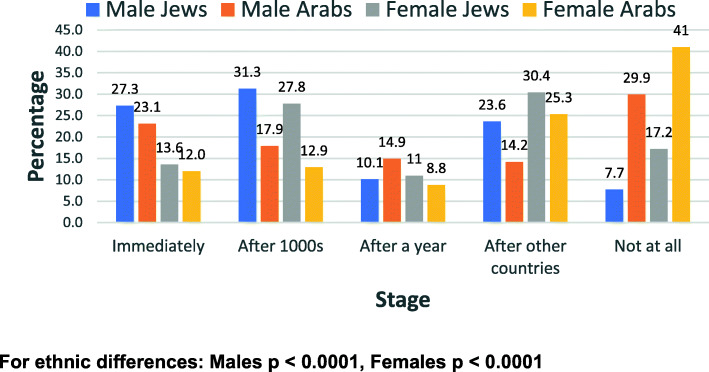
Results: The sample of Arabs was younger than for the Jewish respondents. Among the men, 27.3% of the Jewish and 23.1% of the Arab respondents wanted to be vaccinated immediately, compared with only 13.6% of Jewish women and 12.0% of Arab women. An affirmative answer to the question as to whether they would refuse the vaccine at any stage was given by 7.7% of Jewish men and 29.9% of Arab men, and 17.2% of Jewish women and 41.0% of Arab women. Higher education was associated with less vaccine hesitancy. In multiple logistic regression analysis, the ethnic and gender differences persisted after controlling for age and education. Other factors associated with vaccine hesitancy were the belief that the government restrictions were too lenient and the frequency of socializing prior to the pandemic.
Conclusions: The study revealed a relatively high percentage reported would be reluctant to get vaccinated, prior to the introduction of the vaccine. This was more marked so for Arabs then Jews, and more so for women within the ethnic groups. While this was not a true random sample, the findings are consistent with the large ethnic differences in compliance with the vaccine, currently encountered and reinforce the policy implications for developing effective communication to increase vaccine adherence. Government policies directed at controlling the pandemic should include sector-specific information campaigns, which are tailored to ensure community engagement, using targeted messages to the suspected vaccine hesitant groups. Government ministries, health service providers and local authorities should join hands with civil society organizations to promote vaccine promotion campaigns.
Keywords: Arabs; COVID-19; Education; Ethnic groups; Gender; Jews; Vaccine hesitancy.
Conflict of interest statement
We declare that we do not have any competing interests.
Figures


References
-
- World Health Organisation. Ten threats to global health in 2019. https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-.... Accessed on 29 Jan 2021.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
