

Osteogenesis imperfecta tooth level phenotype analysis: Cross-sectional study
- PMID: 33741542
- PMCID: PMC8278321
- DOI: 10.1016/j.bone.2021.115917
Osteogenesis imperfecta tooth level phenotype analysis: Cross-sectional study
Abstract
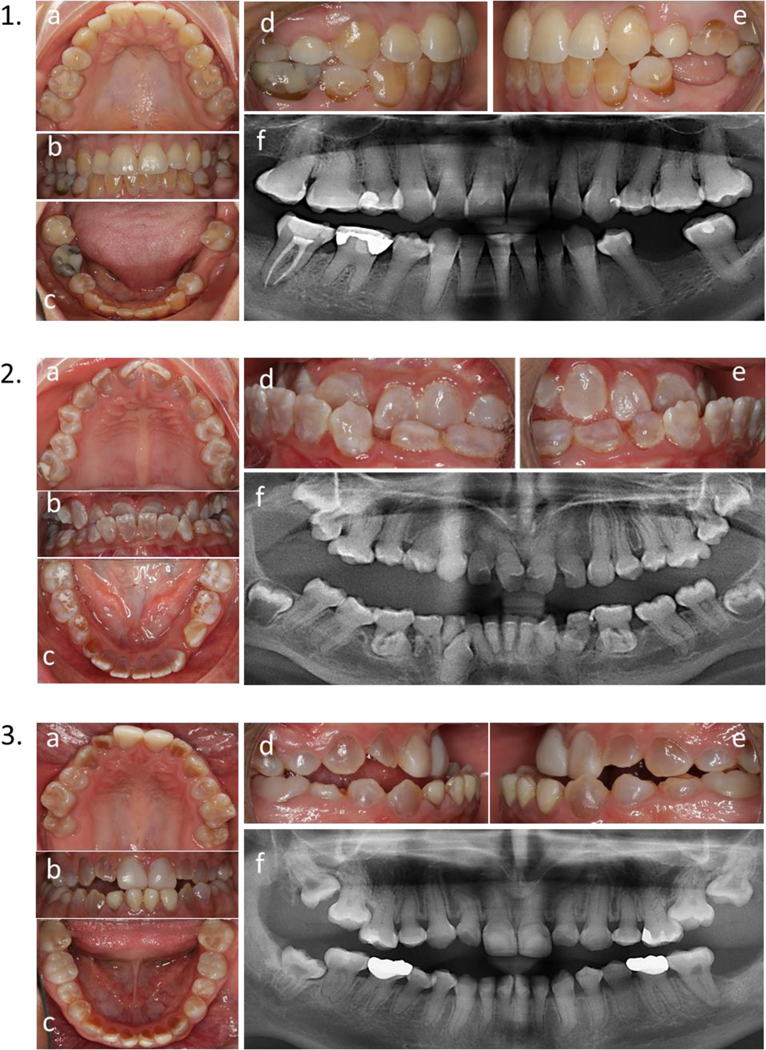
Introduction: Dental anomalies in Osteogenesis imperfecta (OI), such as tooth discoloration, pulp obliteration (calcified dental pulp space), and taurodontism (enlarged dental pulp space) vary between and within patients. To better understand the associations and variations in these anomalies, a cross-sectional study was designed to analyze the dental phenotype in OI patients at the individual tooth type.
Method: A cohort of 171 individuals with OI type I, III and IV, aged 3-55 years, were recruited and evaluated for tooth discoloration, pulp obliteration, and taurodontism at the individual tooth level, using intraoral photographs and panoramic radiographs.
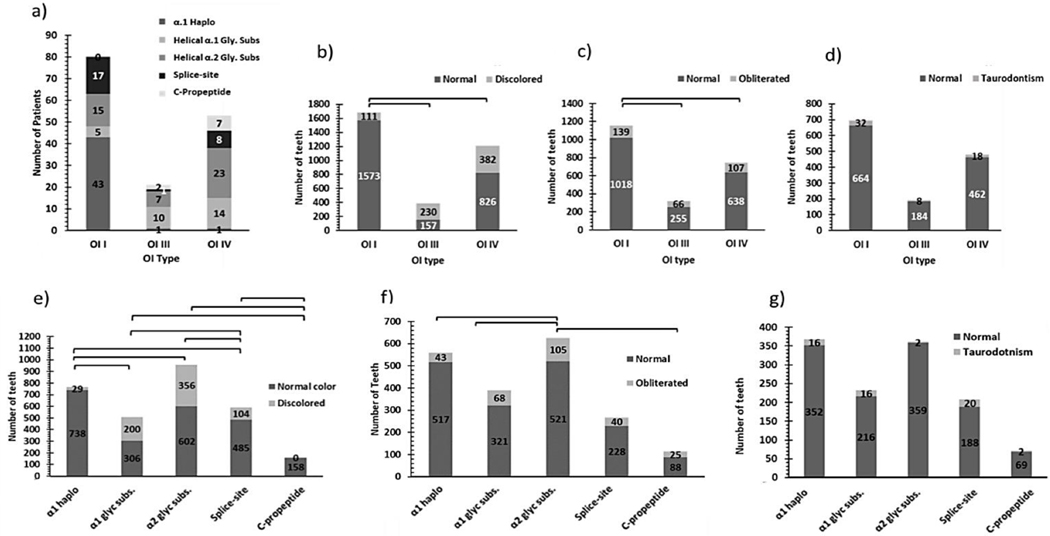
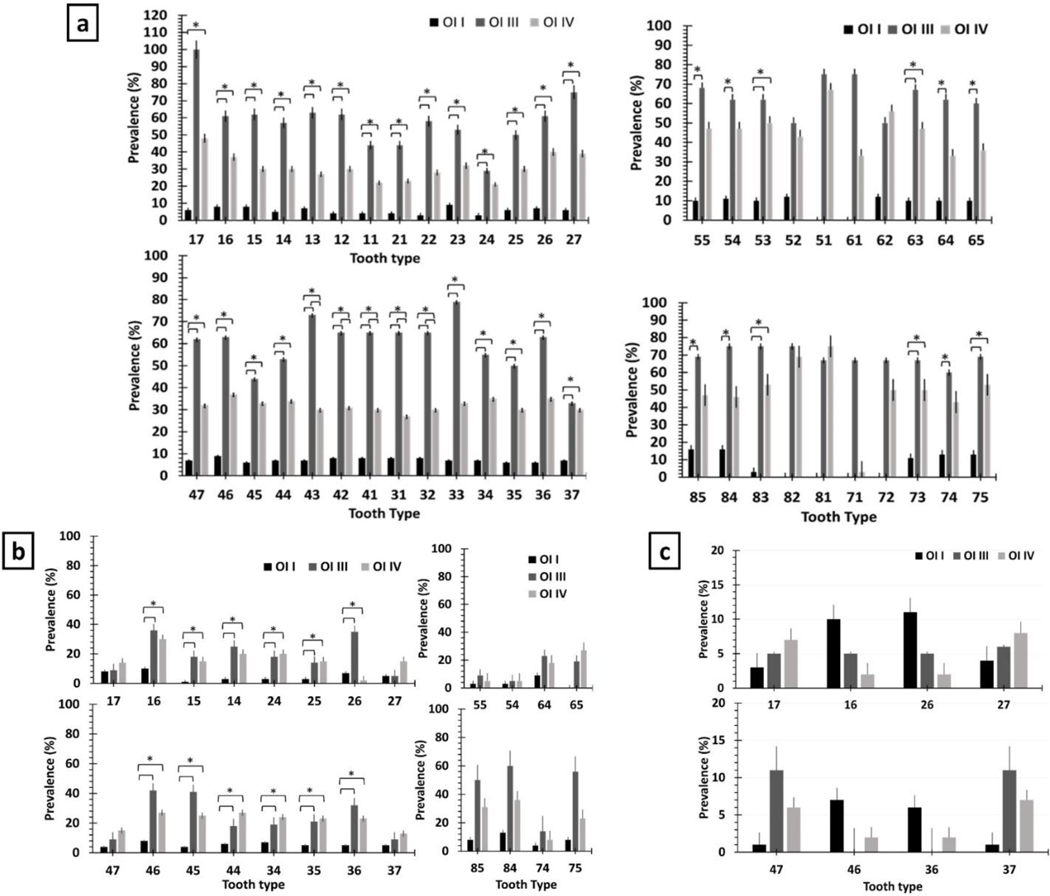
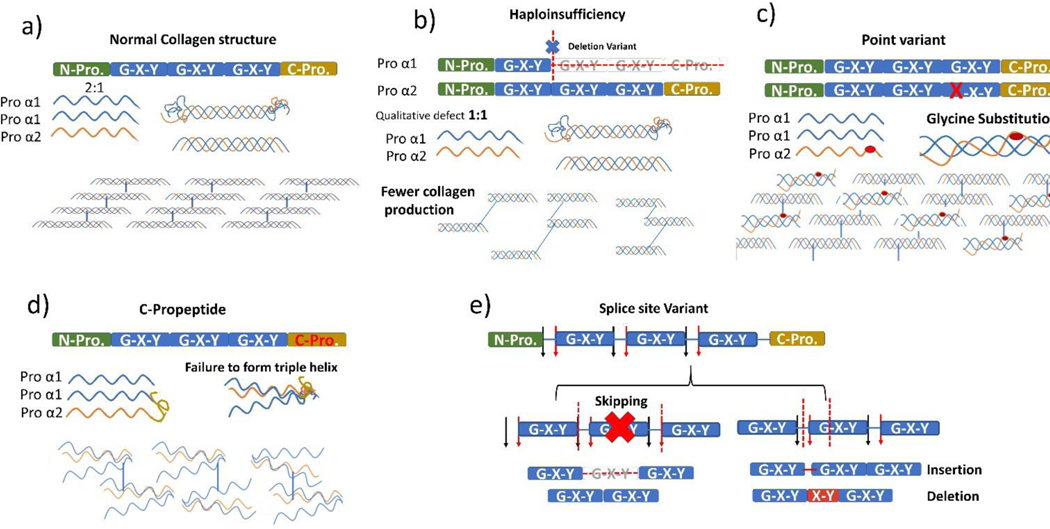
Results: Genetic variants were identified in 154 of the participants. Patients with Helical α1 and α2 glycine substitutions presented the highest prevalence of tooth discoloration, while those with α1 Haploinsufficiency had the lowest (<10%). C-propeptide variants did not cause discoloration but resulted in the highest pulp obliteration prevalence (~%20). The prevalence of tooth discoloration and pulp obliteration was higher in OI types III and IV and increased with age. Tooth discoloration was mainly observed in teeth known to have thinner enamel (i.e. lower anterior), while pulp obliteration was most prevalent in the first molars. A significant association was observed between pulp obliteration and tooth discoloration, and both were associated with a lack of occlusal contact. Taurodontism was only found in permanent teeth and affected mostly first molars, and its prevalence decreased with age.
Conclusion: The dental phenotype evaluation at the tooth level revealed that different genetic variants and associated clinical phenotypes affect each tooth type differently, and genetic variants are better predictors of the dental phenotype than the type of OI. Our results also suggest that tooth discoloration is most likely an optical phenomenon inversely proportional to enamel thickness, and highly associated with pulp obliteration. In turn, pulp obliteration is proportional to patient age, it is associated with malocclusion and likely related to immature progressive dentin deposition. Taurodontism is an isolated phenomenon that is probably associated with delayed pulpal maturation.
Keywords: Connective tissue; Dentin; Dentinogenesis; Oral medicine; Osteogenesis Imperfecta; Tooth abnormalities.
Copyright © 2021. Published by Elsevier Inc.
Conflict of interest statement
We declare no conflict of interest.
Figures

References
-
- Marini JC, Forlino A, Bachinger HP, Bishop NJ, Byers PH, Paepe A, et al. Osteogenesis imperfecta. Nature Reviews Disease Primers. 2017;3:17052. - PubMed
-
- Sillence DO, Rimoin DL. Classification of osteogenesis imperfect. Lancet. 1978;1(8072):1041–2. - PubMed
-
- Trejo P, Rauch F. Osteogenesis imperfecta in children and adolescents-new developments in diagnosis and treatment. Osteoporos Int. 2016:1–11. - PubMed
-
- Rauch F, Glorieux FH. Osteogenesis imperfecta. The Lancet. 2004;363(9418):1377–85. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
