

Pregnancies in Diabetes and Obesity: The Capacity-Load Model of Placental Adaptation
- PMID: 33741605
- PMCID: PMC7980199
- DOI: 10.2337/db20-1111
Pregnancies in Diabetes and Obesity: The Capacity-Load Model of Placental Adaptation
Abstract
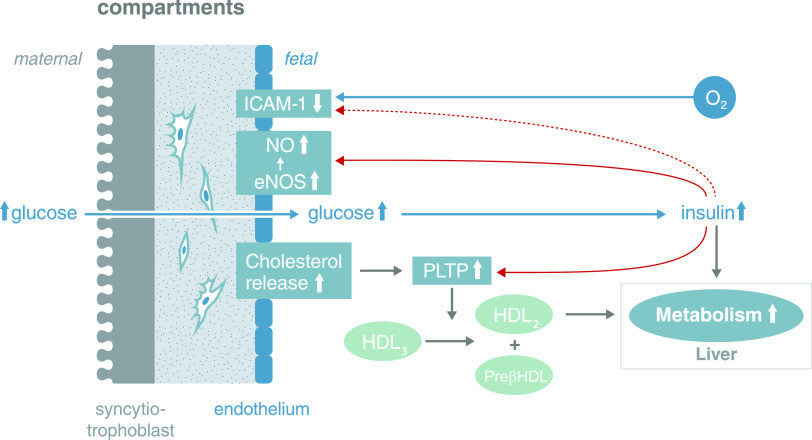
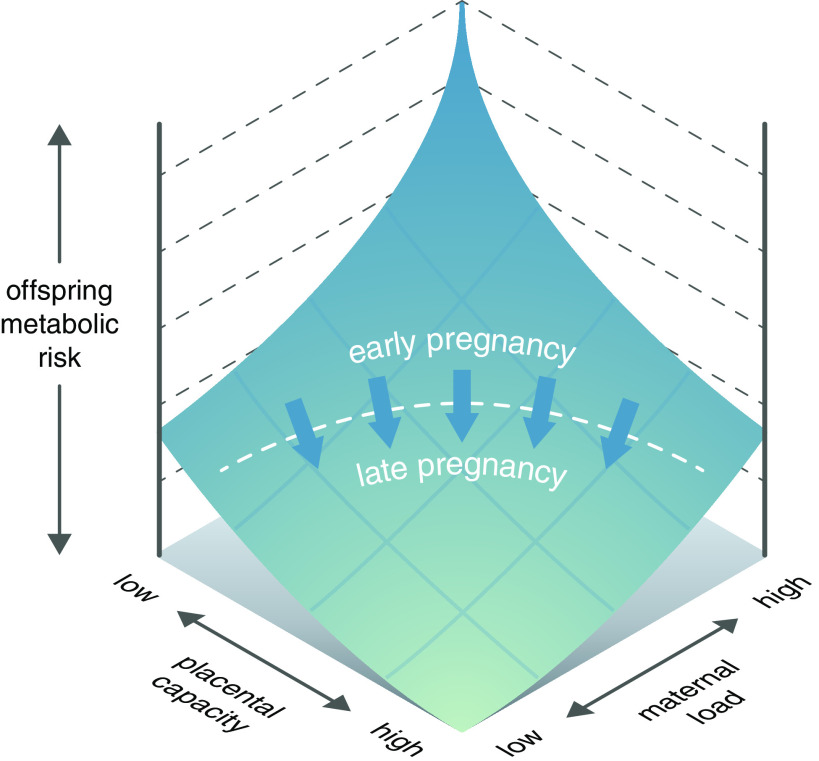
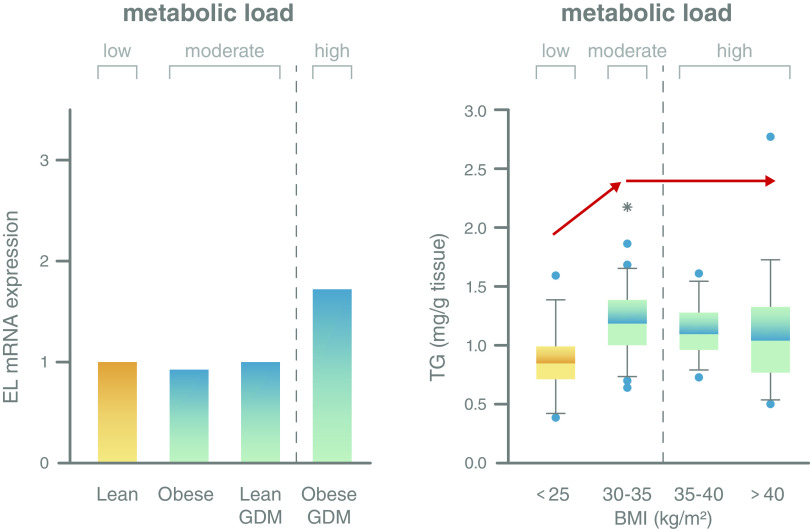
Excess nutritional supply to the growing fetus, resulting from maternal diabetes and obesity, is associated with increased risks of fetal maldevelopment and adverse metabolic conditions in postnatal life. The placenta, interposed between mother and fetus, serves as the gateway between the two circulations and is usually considered to mediate maternal exposures to the fetus through a direct supply line. In this Perspective, however, we argue that the placenta is not an innocent bystander and mounts responses to fetal "signals of distress" to sustain its own adequate function and protect the fetus. We describe several types of protection that the placenta can offer the fetus against maternal metabolic perturbations and offer a theoretical model of how the placenta responds to the intrauterine environment in maternal diabetes and obesity to stabilize the fetal environment. Our approach supports growing calls for early screening and control of pregnancy metabolism to minimize harmful fetal outcomes.
© 2021 by the American Diabetes Association.
Figures
References
-
- Gauster M, Desoye G, Tötsch M, Hiden U. The placenta and gestational diabetes mellitus. Curr Diab Rep 2012;12:16–23 - PubMed
-
- Catalano PM, Thomas A, Huston-Presley L, Amini SB. Phenotype of infants of mothers with gestational diabetes. Diabetes Care 2007;30(Suppl. 2):S156–S160 - PubMed
-
- McIntyre HD, Catalano P, Zhang C, Desoye G, Mathiesen ER, Damm P. Gestational diabetes mellitus. Nat Rev Dis Primers 2019;5:47. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
