

Structural Variants at the BRCA1/2 Loci are a Common Source of Homologous Repair Deficiency in High-grade Serous Ovarian Carcinoma
- PMID: 33741650
- PMCID: PMC7610896
- DOI: 10.1158/1078-0432.CCR-20-4068
Structural Variants at the BRCA1/2 Loci are a Common Source of Homologous Repair Deficiency in High-grade Serous Ovarian Carcinoma
Abstract
Purpose: The abundance and effects of structural variation at BRCA1/2 in tumors are not well understood. In particular, the impact of these events on homologous recombination repair deficiency (HRD) has yet to be demonstrated.
Experimental design: Exploiting a large collection of whole-genome sequencing data from high-grade serous ovarian carcinoma (N = 205) together with matched RNA sequencing for the majority of tumors (N = 150), we have comprehensively characterized mutation and expression at BRCA1/2.
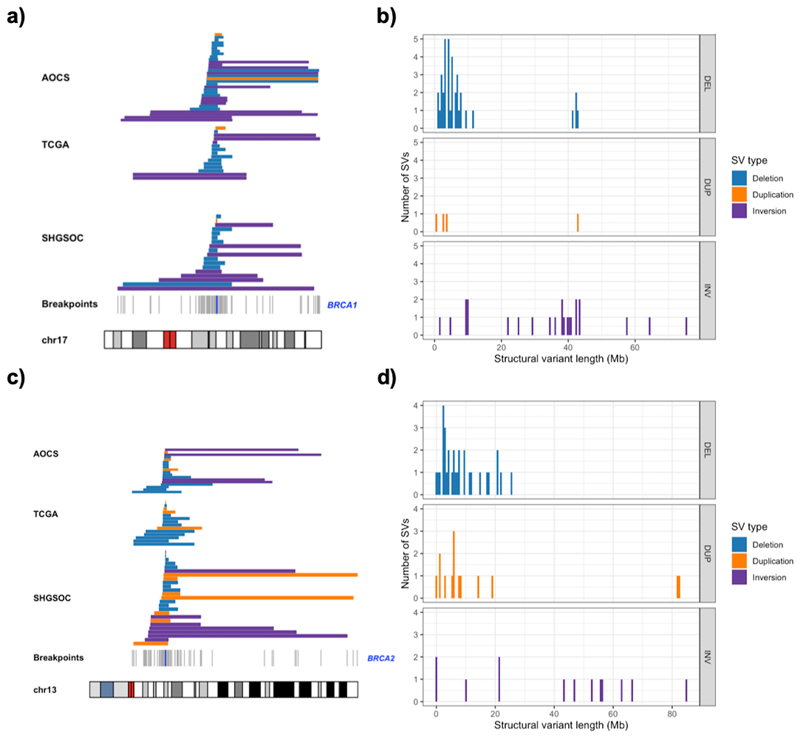
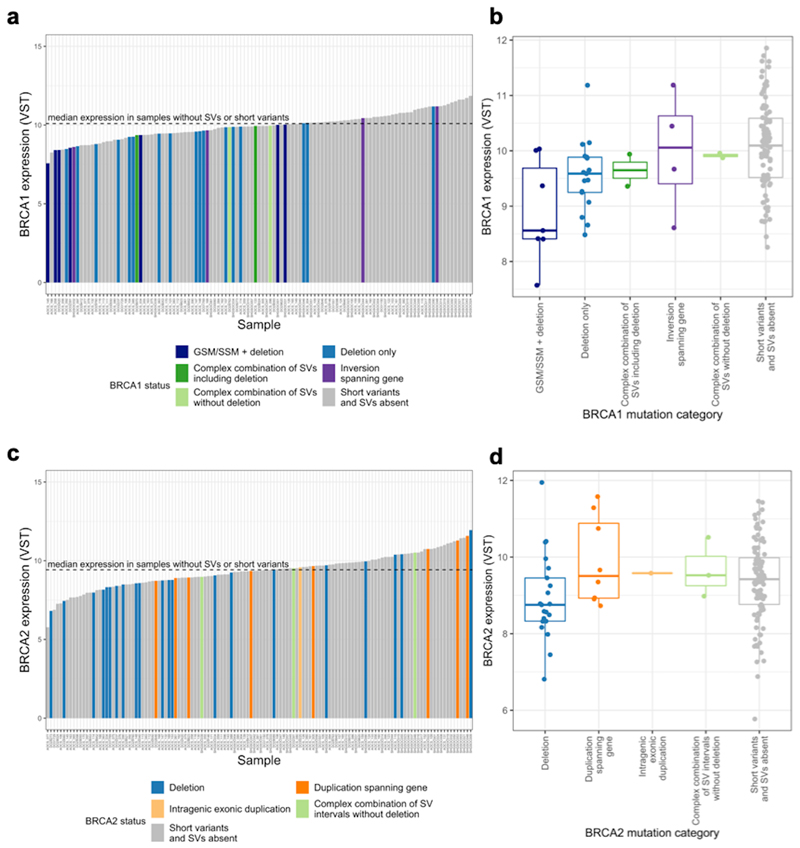
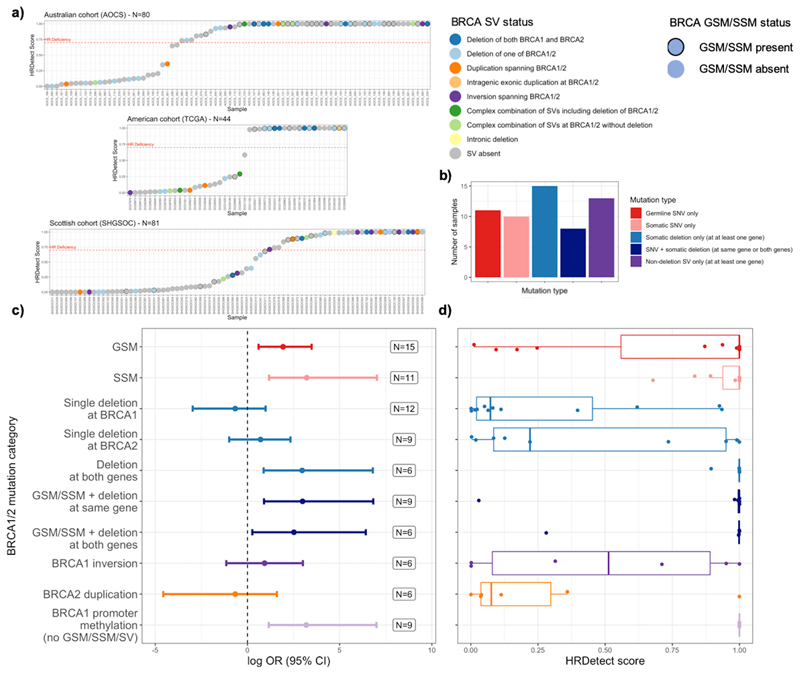
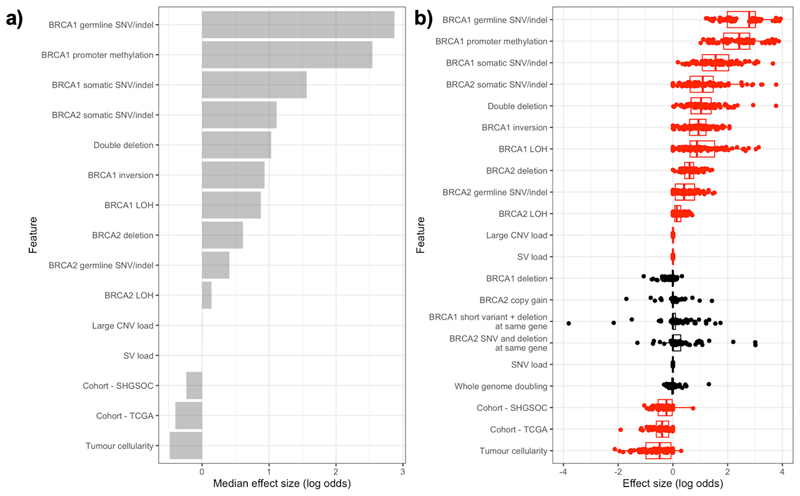
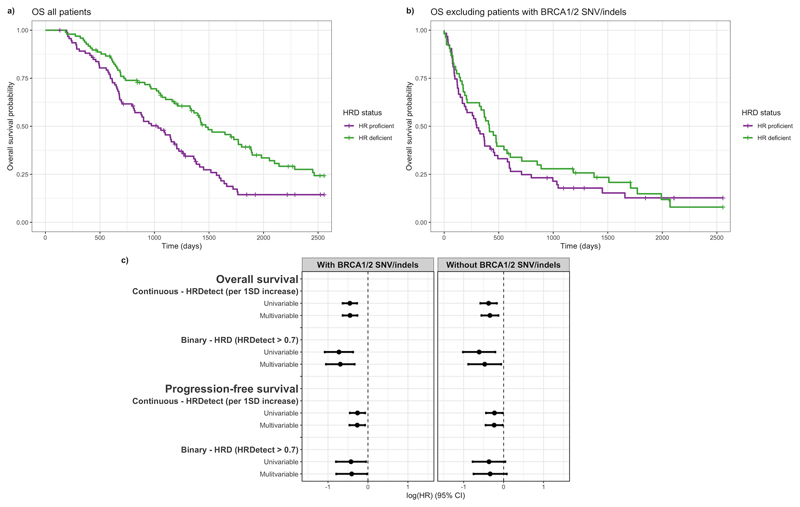
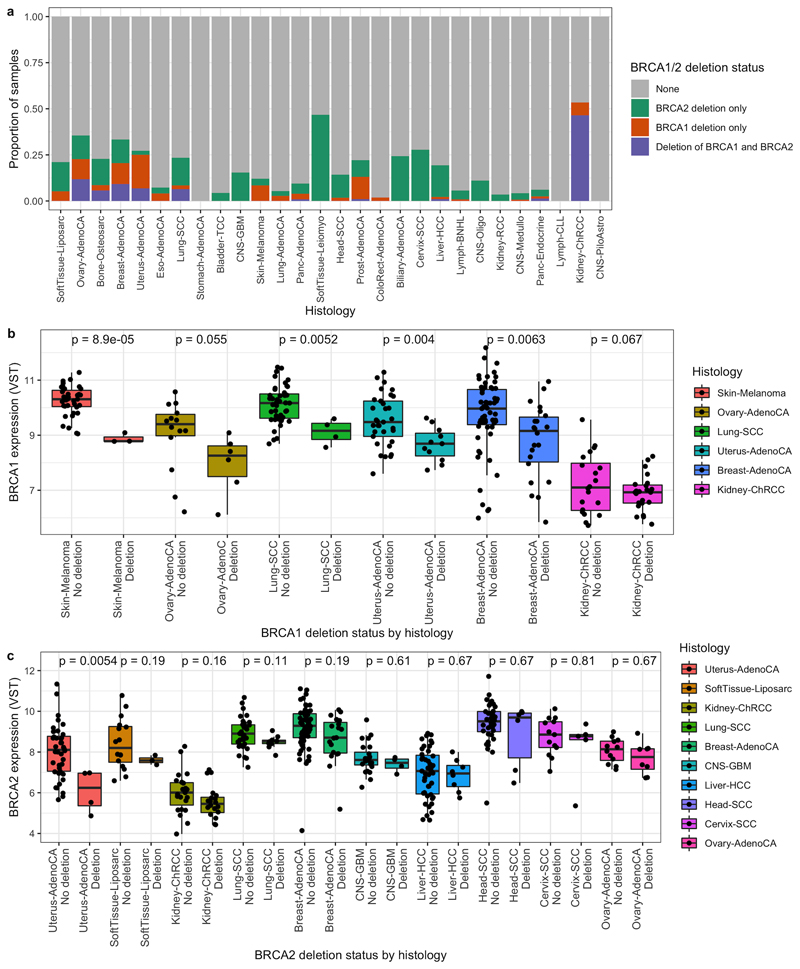
Results: In addition to the known spectrum of short somatic mutations (SSM), we discovered that multi-megabase structural variants (SV) were a frequent, unappreciated source of BRCA1/2 disruption in these tumors, and we found a genome-wide enrichment for large deletions at the BRCA1/2 loci across the cohort. These SVs independently affected a substantial proportion of patients (16%) in addition to those affected by SSMs (24%), conferring HRD and impacting patient survival. We also detail compound deficiencies involving SSMs and SVs at both loci, demonstrating that the strongest risk of HRD emerges from combined SVs at both BRCA1 and BRCA2 in the absence of SSMs. Furthermore, these SVs are abundant and disruptive in other cancer types.
Conclusions: These results extend our understanding of the mutational landscape underlying HRD, increase the number of patients predicted to benefit from therapies exploiting HRD, and suggest there is currently untapped potential in SV detection for patient stratification.
©2021 American Association for Cancer Research.
Conflict of interest statement
J.C.B, A.M and B.D are employees and stock holders of AstraZeneca. I.A.M is on the advisory boards for Clovis Oncology, Tesaro, AstraZeneca, Carrick Therapeutics, Roche and ScanCell. I.A.M also benefits from institutional funding from AstraZeneca. C.G. has received research funding from AstraZeneca, Aprea, Nucana, Tesaro, GSK and Novartis; honoraria/consultancy fees from Roche, AstraZeneca, Tesaro, GSK, Nucana, MSD, Clovis, Foundation One, Sierra Oncology and Cor2Ed; and is named on issued/pending patents relating to predicting treatment response in ovarian cancer unrelated to this work. R.G is or has been on the advisory boards of AstraZeneca, GSK, Tesaro and Clovis; has received speaker fees and funding to attend medical conferences from GSK and Tesaro and is a UK co-ordinating investigator or site principal investigator for studies sponsored by Astrazeneca, GSK, Pfizer and Clovis. F.N has been or is a site principal investigator for studies sponsored by AstraZeneca and Clovis. P.R has received research funding from AstraZeneca and Tesaro and honoraria/consultancy fees from AstraZeneca and GSK.
Figures
References
-
- Patch A-M, et al. Whole-genome characterization of chemoresistant ovarian cancer. Nature. 2015;521:489–494. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- C29717/A18484/CRUK_/Cancer Research UK/United Kingdom
- A23526/CRUK_/Cancer Research UK/United Kingdom
- MC_UU_00007/16/MRC_/Medical Research Council/United Kingdom
- MR/R026017/1/MRC_/Medical Research Council/United Kingdom
- MC_PC_15080/MRC_/Medical Research Council/United Kingdom
- C596/A20921/CRUK_/Cancer Research UK/United Kingdom
- C29717/A17263/CRUK_/Cancer Research UK/United Kingdom
- A17263/CRUK_/Cancer Research UK/United Kingdom
- C596/A18076/CRUK_/Cancer Research UK/United Kingdom
- 103721/Z/14/Z/WT_/Wellcome Trust/United Kingdom
- WT_/Wellcome Trust/United Kingdom
- A18484/CRUK_/Cancer Research UK/United Kingdom
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
