

Renal Cell Carcinoma and Kidney Transplantation: A Narrative Review
- PMID: 33741842
- PMCID: PMC8667800
- DOI: 10.1097/TP.0000000000003762
Renal Cell Carcinoma and Kidney Transplantation: A Narrative Review
Abstract
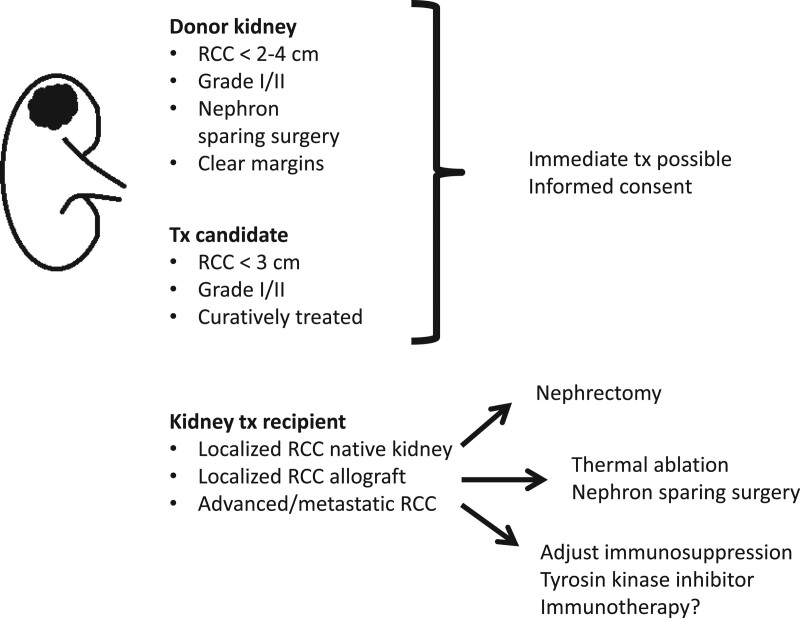
Kidney transplant recipients (KTRs) are at increased risk of developing renal cell carcinoma (RCC). The cancer can be encountered at different steps in the transplant process. RCC found during work-up of a transplant candidate needs treatment and to limit the risk of recurrence usually a mandatory observation period before transplantation is recommended. An observation period may be omitted for candidates with incidentally discovered and excised small RCCs (<3 cm). Likewise, RCC in the donor organ may not always preclude usage if tumor is small (<2 to 4 cm) and removed with clear margins before transplantation. After transplantation, 90% of RCCs are detected in the native kidneys, particularly if acquired cystic kidney disease has developed during prolonged dialysis. Screening for RCC after transplantation has not been found cost-effective. Treatment of RCC in KTRs poses challenges with adjustments of immunosuppression and oncologic treatments. For localized RCC, excision or nephrectomy is often curative. For metastatic RCC, recent landmark trials in the nontransplanted population demonstrate that immunotherapy combinations improve survival. Dedicated trials in KTRs are lacking. Case series on immune checkpoint inhibitors in solid organ recipients with a range of cancer types indicate partial or complete tumor response in approximately one-third of the patients at the cost of rejection developing in ~40%.
Copyright © 2021 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Cohen HT, McGovern FJ. Renal-cell carcinoma. N Engl J Med. 2005;353:2477–2490. - PubMed
-
- Griffith JJ, Amin KA, Waingankar N, et al. . Solid renal masses in transplanted allograft kidneys: a closer look at the epidemiology and management. Am J Transplant. 2017;17:2775–2781. - PubMed
-
- Ljungberg B, Albiges L, Bensalah K, et al. . Renal cell carcinoma, European Association of Urology (EAU) Guidelines. 2020. Available at http://uroweb.org/guidelines/compilations-of-all-guidelines/. Accessed October 11, 2020.
-
- Amato RJ. Chemotherapy for renal cell carcinoma. Semin Oncol. 2000;27:177–186. - PubMed
-
- Bumpus HC. The apparent disappearance of pulmonary metastasis in a case of hypernephroma following nephrectomy. J Urol. 1928;20:185–191.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
