

Clonal architecture in mesothelioma is prognostic and shapes the tumour microenvironment
- PMID: 33741915
- PMCID: PMC7979861
- DOI: 10.1038/s41467-021-21798-w
Clonal architecture in mesothelioma is prognostic and shapes the tumour microenvironment
Erratum in
-
Author Correction: Clonal architecture in mesothelioma is prognostic and shapes the tumour microenvironment.Nat Commun. 2021 Jun 7;12(1):3569. doi: 10.1038/s41467-021-23867-6. Nat Commun. 2021. PMID: 34099722 Free PMC article. No abstract available.
Abstract
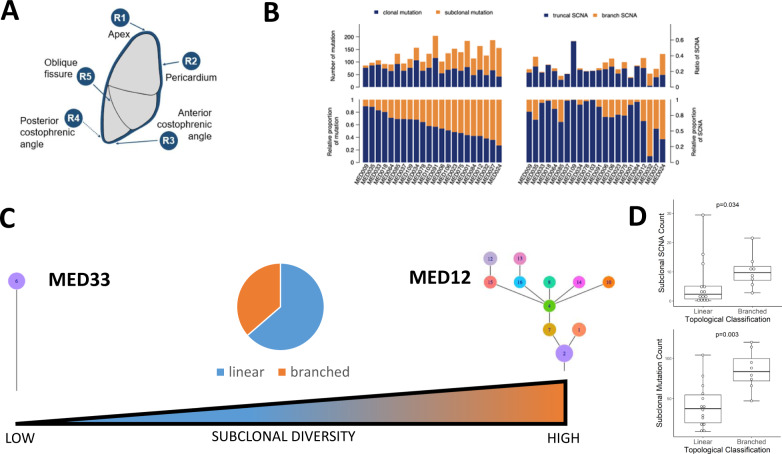
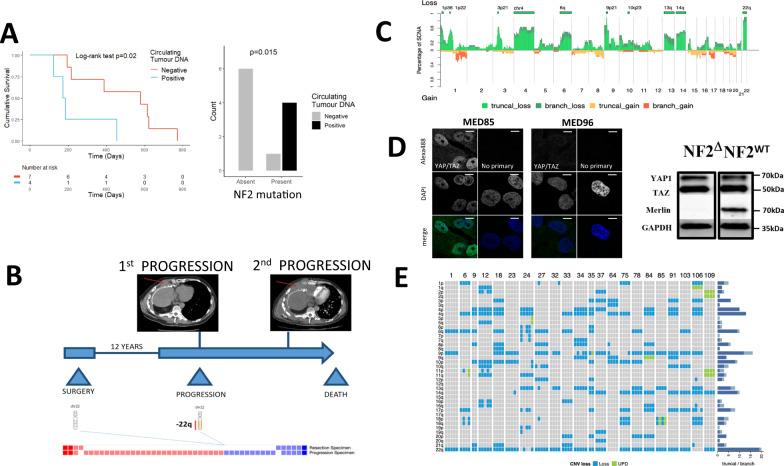
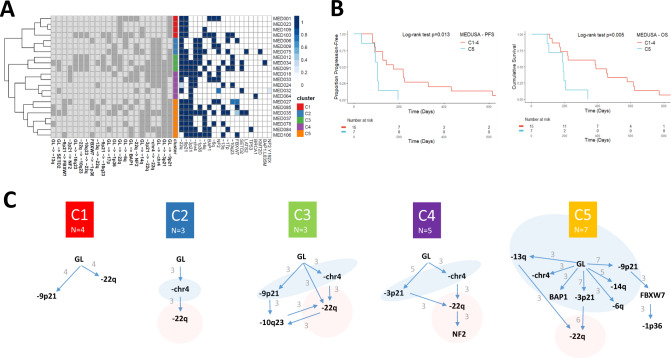
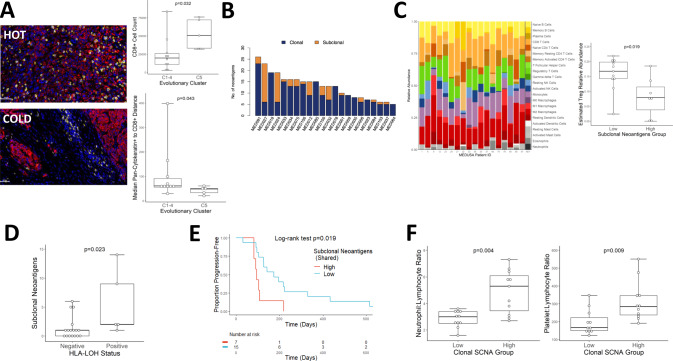
Malignant Pleural Mesothelioma (MPM) is typically diagnosed 20-50 years after exposure to asbestos and evolves along an unknown evolutionary trajectory. To elucidate this path, we conducted multi-regional exome sequencing of 90 tumour samples from 22 MPMs acquired at surgery. Here we show that exomic intratumour heterogeneity varies widely across the cohort. Phylogenetic tree topology ranges from linear to highly branched, reflecting a steep gradient of genomic instability. Using transfer learning, we detect repeated evolution, resolving 5 clusters that are prognostic, with temporally ordered clonal drivers. BAP1/-3p21 and FBXW7/-chr4 events are always early clonal. In contrast, NF2/-22q events, leading to Hippo pathway inactivation are predominantly late clonal, positively selected, and when subclonal, exhibit parallel evolution indicating an evolutionary constraint. Very late somatic alteration of NF2/22q occurred in one patient 12 years after surgery. Clonal architecture and evolutionary clusters dictate MPM inflammation and immune evasion. These results reveal potentially drugable evolutionary bottlenecking in MPM, and an impact of clonal architecture on shaping the immune landscape, with potential to dictate the clinical response to immune checkpoint inhibition.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Kircheva DY, et al. Specimen weight and volume: important predictors of survival in malignant pleural mesothelioma. Eur. J. Cardiothorac. Surg. 2016;49:1642–1647. - PubMed
-
- Baas P, et al. First-line nivolumab plus ipilimumab in unresectable malignant pleural mesothelioma (CheckMate 743): a multicentre, randomised, open-label, phase 3 trial. The Lancet. 2021;397:375–386. - PubMed
-
- Yap TA, Aerts JG, Popat S, Fennell DA. Novel insights into mesothelioma biology and implications for therapy. Nat. Rev. Cancer. 2017;17:475–488. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
