

Circulating stromal cells in resectable pancreatic cancer correlates to pathological stage and predicts for poor clinical outcomes
- PMID: 33742084
- PMCID: PMC7979885
- DOI: 10.1038/s41698-021-00161-8
Circulating stromal cells in resectable pancreatic cancer correlates to pathological stage and predicts for poor clinical outcomes
Abstract
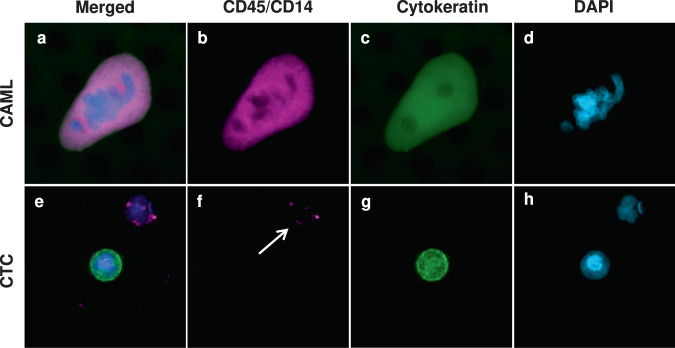
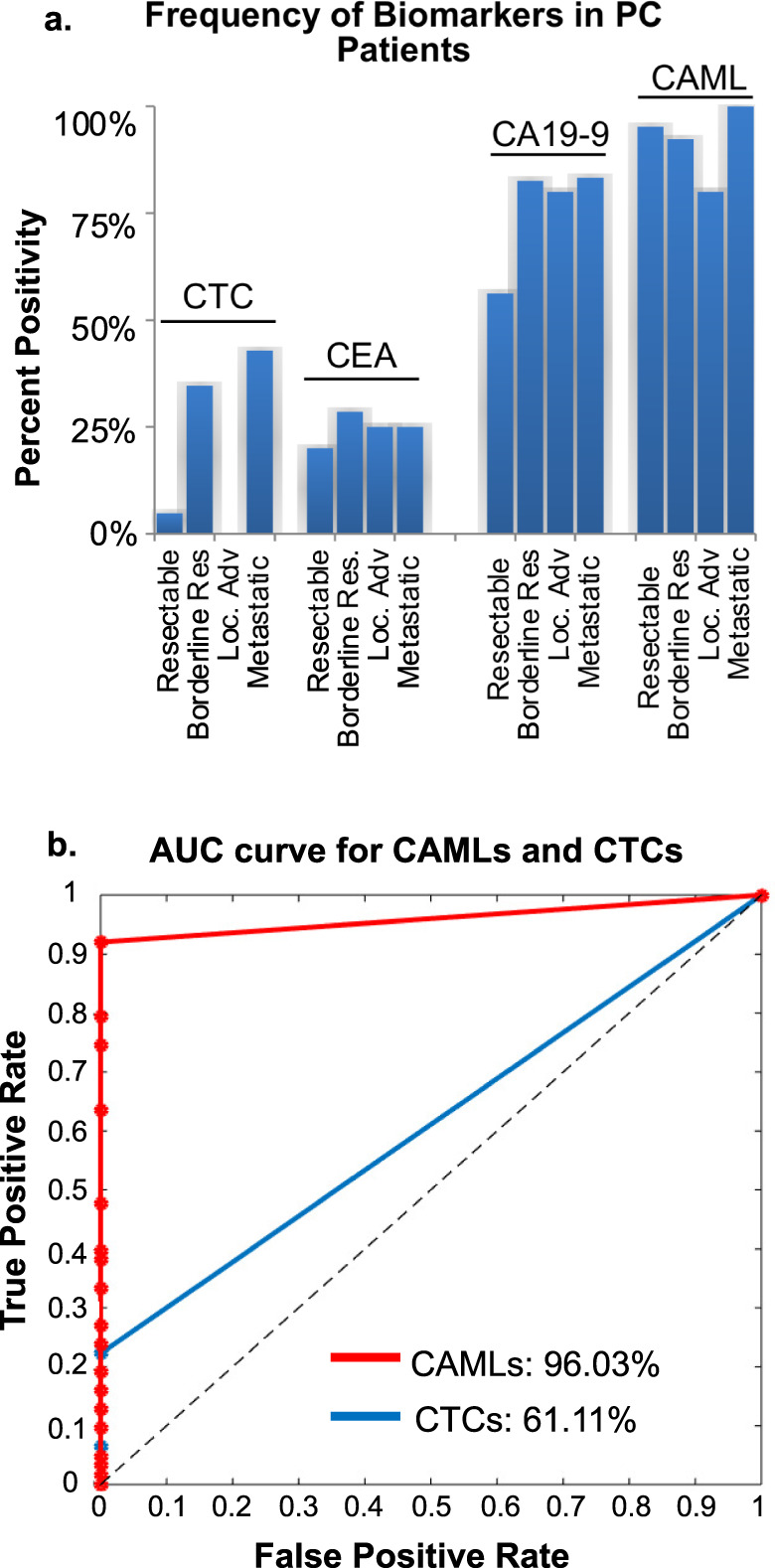
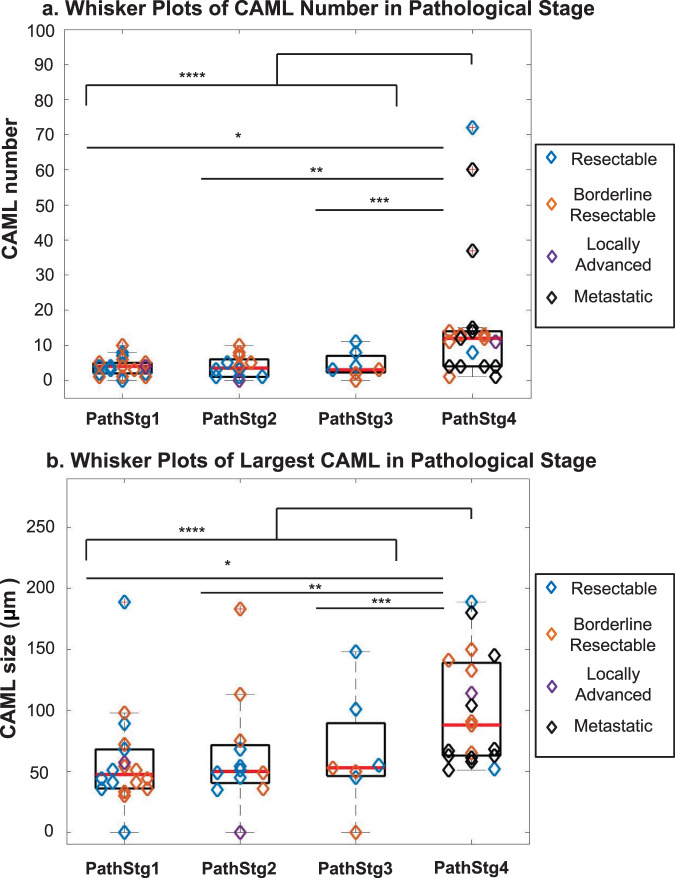
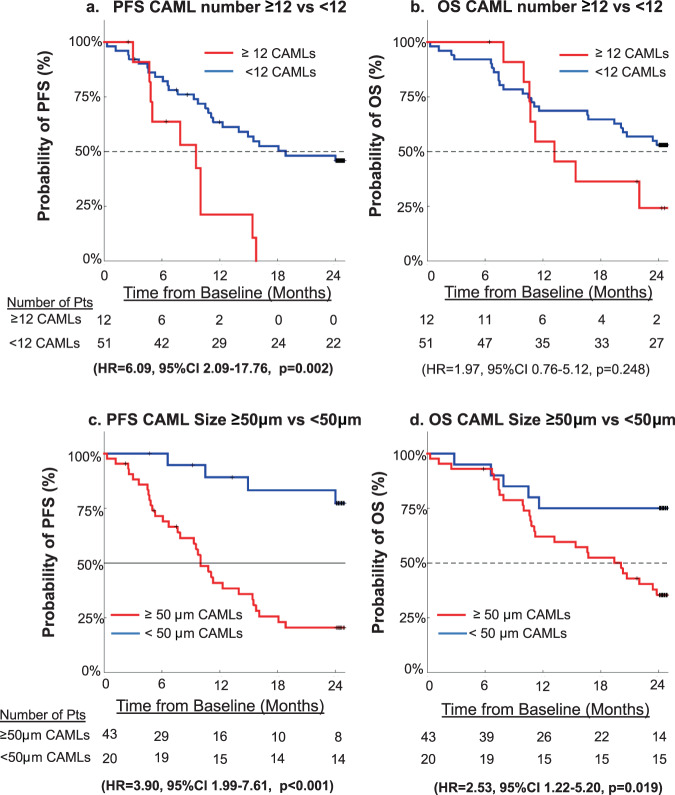
Pancreatic cancer (PC) is notoriously difficult to diagnosis and properly stage resulting in incorrect primary treatment. Diagnostic and prognostic biomarkers are desperately needed to more accurately stage patients and select proper treatments. Recently, a newly discovered circulating stromal cell, i.e. cancer associated macrophage-like cell (CAML), was found to accurately identify solid cancers and predict for worse prognosis. In this pilot study, blood samples were procured from 63 PC patients prior to start of therapeutic intent. CAMLs were found in 95% of samples tested, with ≥12 CAMLs/7.5 mL and ≥50 µm CAMLs both predicting for advanced pathological stage and progression free survival. These data suggest that CAML assessment prior to treatment of PC predicts patients with under-staged disease and with more aggressive PC less likely to respond to standard of care treatment.
Conflict of interest statement
The authors declare no competing non-financial interests but the following competing financial interests. D.L.A. and C.M.T. are employees of Creatv MicroTech, own stocks in Creatv MicroTech Inc. and have filed patent applications. K.P.G. is an independent contractor for Creatv MicroTech, Inc. The remaining authors have no other conflicts to report.
Figures
References
-
- Howlader N. N. A. et al. SEER Cancer Statistics Review, 1975–2016, https://seer.cancer.gov/csr/1975_2016/ (2019).
-
- Stuart H, et al. Significant upstaging of patients with stage I pancreatic cancer from clinical to pathologic staging. J. Clin. Oncol. 2017;35:349–349. doi: 10.1200/JCO.2017.35.4_suppl.349. - DOI
LinkOut - more resources
Full Text Sources
Other Literature Sources
