

Comparative Effectiveness of a Complex Care Program for High-Cost/High-Need Patients: a Retrospective Cohort Study
- PMID: 33742306
- PMCID: PMC8298622
- DOI: 10.1007/s11606-021-06676-x
Comparative Effectiveness of a Complex Care Program for High-Cost/High-Need Patients: a Retrospective Cohort Study
Abstract
Background: High-cost/high-need (HCHN) adults and the healthcare systems that provide their care may benefit from a new patient-centered model of care involving a dedicated physician and nurse team who coordinate both clinical and social services for a small patient panel.
Objective: Evaluate the impact of a Complex Care Program (CCP) on likelihood of patient survival and hospital admission in 180 days following empanelment to the CCP.
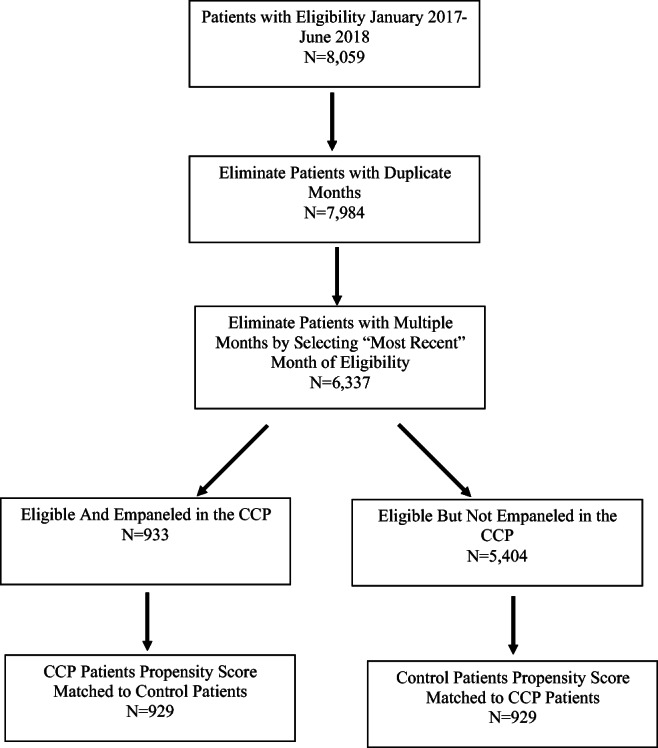
Design: Retrospective cohort study using a quasi-experimental design with CCP patients propensity score matched to a concurrent control group of eligible but unempaneled patients.
Setting: Kaiser Permanente Mid-Atlantic States (KPMAS) during 2017-2018.
Participants: Nine hundred twenty-nine CCP patients empaneled January 2017-June 2018, 929 matched control patients for the same period.
Interventions: The KPMAS CCP is a new program consisting of 8 teams each staffed by a physician and nurse who coordinate care across a continuum of specialty care, tertiary care, and community services for a panel of 200 patients with advanced clinical disease and recent hospitalizations.
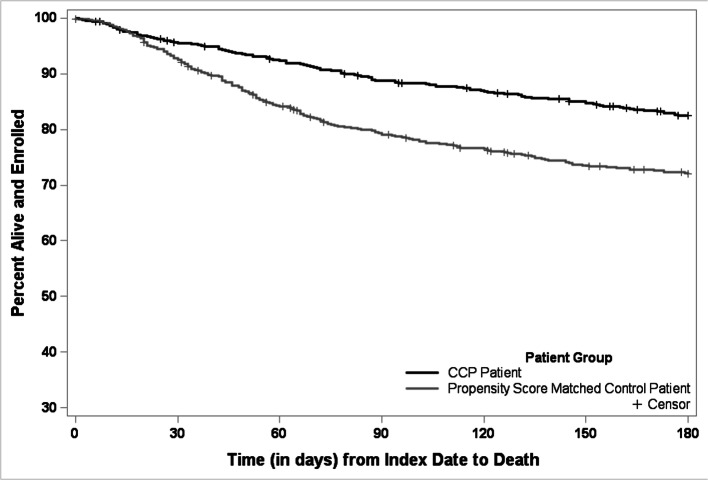
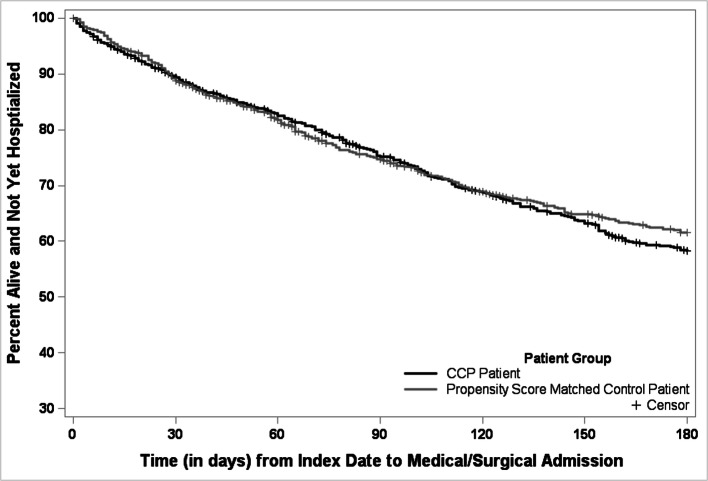
Main outcomes: Time to death and time to first hospital admission in the 180 days following empanelment or eligibility.
Results: Compared to matched control patients, CCP patients had prolonged time to death (hazard ratio [HR]: 0.577, 95% CI: 0.474, 0.704), and CCP decedents had longer survival (median days 69.5 vs. 53.0, p=0.03). CCP patients had similar time to hospital admission (HR: 1.081, 95% CI: 0.930, 1.258), with similar results when adjusting for competing risk of death (HR: 1.062, 95% CI: 0.914, 1.084).
Limitations: Non-randomized intervention; single healthcare system; patient eligibility limited to specific conditions.
Conclusion: The KPMAS CCP was associated with significantly reduced short-term mortality risk for eligible patients who volunteered to participate in this intervention.
© 2021. Society of General Internal Medicine.
Conflict of interest statement
The authors have no financial conflicts of interest to disclose. Drs. McCarthy, Mendiratta, and Roblin are affiliated with the medical group which designed and implemented the intervention.
Figures
Similar articles
-
Community-based care for the specialized management of heart failure: an evidence-based analysis.Ont Health Technol Assess Ser. 2009;9(17):1-42. Epub 2009 Nov 1. Ont Health Technol Assess Ser. 2009. PMID: 23074521 Free PMC article.
-
A Multigene Signature Based on Cell Cycle Proliferation Improves Prediction of Mortality Within 5 Yr of Radical Nephrectomy for Renal Cell Carcinoma.Eur Urol. 2018 May;73(5):763-769. doi: 10.1016/j.eururo.2017.12.002. Epub 2017 Dec 14. Eur Urol. 2018. PMID: 29249291
-
Association of Ambulatory Hemodynamic Monitoring of Heart Failure With Clinical Outcomes in a Concurrent Matched Cohort Analysis.JAMA Cardiol. 2019 Jun 1;4(6):556-563. doi: 10.1001/jamacardio.2019.1384. JAMA Cardiol. 2019. PMID: 31090869 Free PMC article.
-
Systematic reviews of the effectiveness of day care for people with severe mental disorders: (1) acute day hospital versus admission; (2) vocational rehabilitation; (3) day hospital versus outpatient care.Health Technol Assess. 2001;5(21):1-75. doi: 10.3310/hta5210. Health Technol Assess. 2001. PMID: 11532238 Review.
-
Endovascular stent grafting and open surgical replacement for chronic thoracic aortic aneurysms: a systematic review and prospective cohort study.Health Technol Assess. 2022 Jan;26(6):1-166. doi: 10.3310/ABUT7744. Health Technol Assess. 2022. PMID: 35094747
Cited by
-
Identifying High-Cost, High-Need Patients in a Network of Community Hospitals.J Prim Care Community Health. 2024 Jan-Dec;15:21501319241233410. doi: 10.1177/21501319241233410. J Prim Care Community Health. 2024. PMID: 38400584 Free PMC article.
References
-
- Cohen SB. The Concentration and Persistence in the Level of Health Expenditures over Time: Estimates for the U.S. Population, 2011-2012. Statistical Brief #449 (Medical Expenditure Panel Survey (US)) [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US). - PubMed
-
- Blumenthal D, Abrams MK. Tailoring complex care management for high-need, high-cost patients. JAMA. 2016;316(16):1657–1658. - PubMed
-
- Blumenthal D, Chernof B, Fulmer T, Lumpkin J, Selberg J. Caring for high-need, high-cost patients: An Urgent priority. New Engl J Med. 2016;375(10):909–911. - PubMed
-
- Cross DA, Cohen GR, Lemak CH, Adler-Milstein J. Outcomes for high-needs patients: Practices with a higher proportion of these patients have an edge. Health Aff. 2017;36(3):476–484. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
