

Interhospital referral of colorectal cancer patients: a Dutch population-based study
- PMID: 33743051
- PMCID: PMC8195929
- DOI: 10.1007/s00384-021-03881-2
Interhospital referral of colorectal cancer patients: a Dutch population-based study
Abstract
Purpose: Interhospital referral is a consequence of centralization of complex oncological care but might negatively impact waiting time, a quality indicator in the Netherlands. This study aims to evaluate characteristics and waiting times of patients with primary colorectal cancer who are referred between hospitals.
Methods: Data were extracted from the Dutch ColoRectal Audit (2015-2019). Waiting time between first tumor-positive biopsy until first treatment was compared between subgroups stratified for referral status, disease stage, and type of hospital.
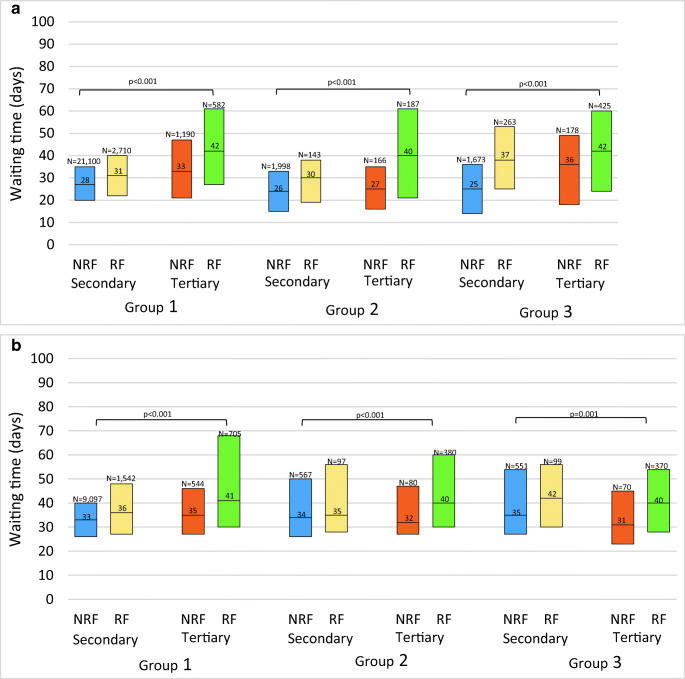
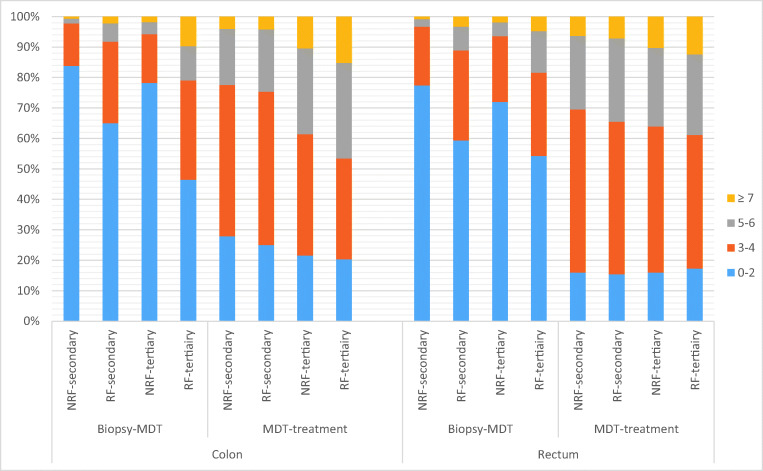
Results: In total, 46,561 patients were included. Patients treated for colon or rectal cancer in secondary care hospitals were referred in 12.2% and 14.7%, respectively. In tertiary care hospitals, corresponding referral rates were 43.8% and 66.4%. Referred patients in tertiary care hospitals were younger, but had a more advanced disease stage, and underwent more often multivisceral resection and simultaneous metastasectomy than non-referred patients in secondary care hospitals (p<0.001). Referred patients were more often treated within national quality standards for waiting time compared to non-referred patients (p<0.001). For referred patients, longer waiting times prior to MDT were observed compared to non-referred patients within each hospital type, although most time was spent post-MDT.
Conclusion: A large proportion of colorectal cancer patients that are treated in tertiary care hospitals are referred from another hospital but mostly treated within standards for waiting time. These patients are younger but often have a more advanced disease. This suggests that these patients are willing to travel more but also reflects successful centralization of complex oncological patients in the Netherlands.
Keywords: Centralization; Colorectal cancer care; Interhospital referral; Waiting time.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
[Surgery for colorectal cancer since the introduction of the Netherlands national screening programmeInvestigations into changes in number of resections and waiting times for surgery].Ned Tijdschr Geneeskd. 2017;161:D997. Ned Tijdschr Geneeskd. 2017. PMID: 28325161 Dutch.
-
The selection process can improve the outcome in locally advanced and recurrent colorectal cancer: activity and results of a dedicated multidisciplinary colorectal cancer centre.Colorectal Dis. 2017 Apr;19(4):331-338. doi: 10.1111/codi.13517. Colorectal Dis. 2017. PMID: 27629565
-
Postoperative Outcomes of Screen-Detected vs Non-Screen-Detected Colorectal Cancer in the Netherlands.JAMA Surg. 2018 Dec 1;153(12):e183567. doi: 10.1001/jamasurg.2018.3567. Epub 2018 Dec 19. JAMA Surg. 2018. PMID: 30285063 Free PMC article.
-
Surgical treatment of pulmonary metastases in the Netherlands: data from the Dutch Lung Cancer Audit for Surgery.Eur J Cardiothorac Surg. 2020 Oct 1;58(4):768-774. doi: 10.1093/ejcts/ezaa090. Eur J Cardiothorac Surg. 2020. PMID: 32282876
-
The standardised mortality ratio is unreliable for assessing quality of care in rectal cancer.Neth J Med. 2013 May;71(4):209-14. Neth J Med. 2013. PMID: 23723118
References
-
- Risberg T, Sørbye SW, Norum J, Wist EA. Diagnostic delay causes more psychological distress in female than in male cancer patients. Anticancer Research. 1996;16(2):995–1000. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
