

Longitudinal associations between exposure to anesthesia and neurocognitive functioning in pediatric medulloblastoma
- PMID: 33743477
- PMCID: PMC8087638
- DOI: 10.1016/j.ejca.2021.02.010
Longitudinal associations between exposure to anesthesia and neurocognitive functioning in pediatric medulloblastoma
Abstract
Aim: To examine whether anesthesia exposure is associated with neurocognitive decline in pediatric medulloblastoma.
Methods: Patients were treated at St. Jude Children's Research Hospital and completed ≥2 protocol-directed neurocognitive assessments (n = 107) as part of a multisite clinical trial for pediatric medulloblastoma (NCT00085202). Patients received risk-adapted craniospinal photon irradiation, followed by four cycles of high-dose chemotherapy and stem cell rescue. Neurocognitive testing was completed at study baseline (after surgery and <2 weeks of starting radiation therapy) and annually for 5 years. Data on anesthesia exposure during treatment was abstracted from medical records.
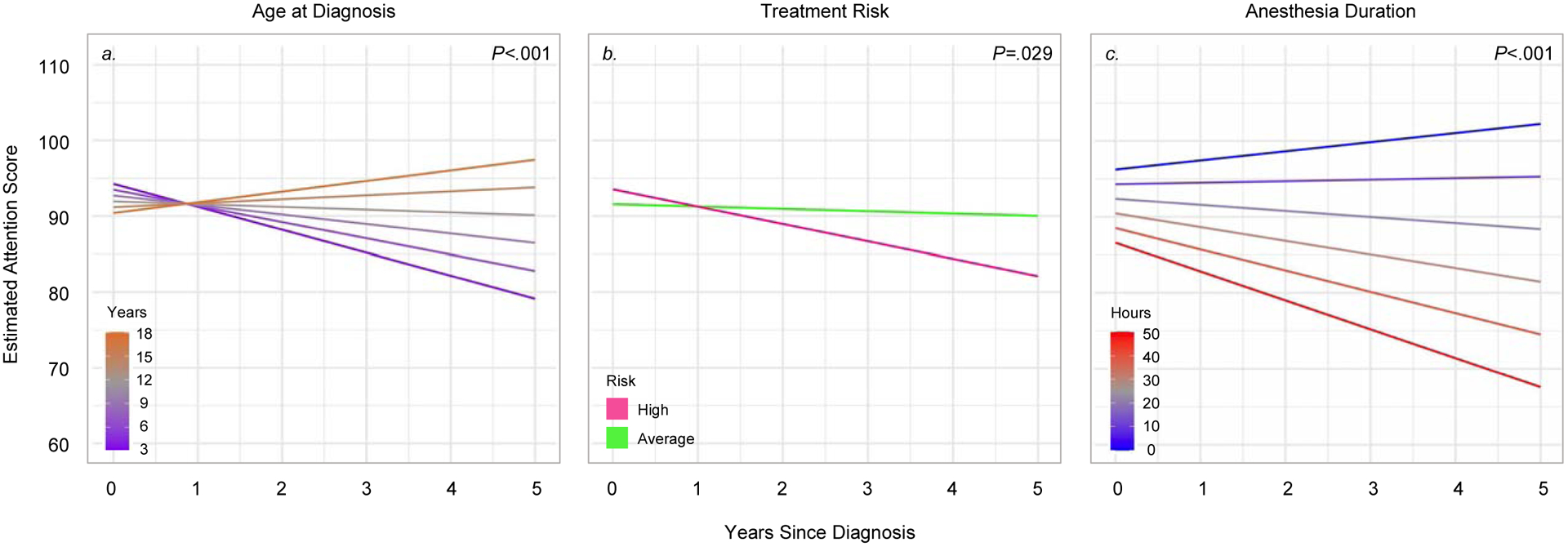
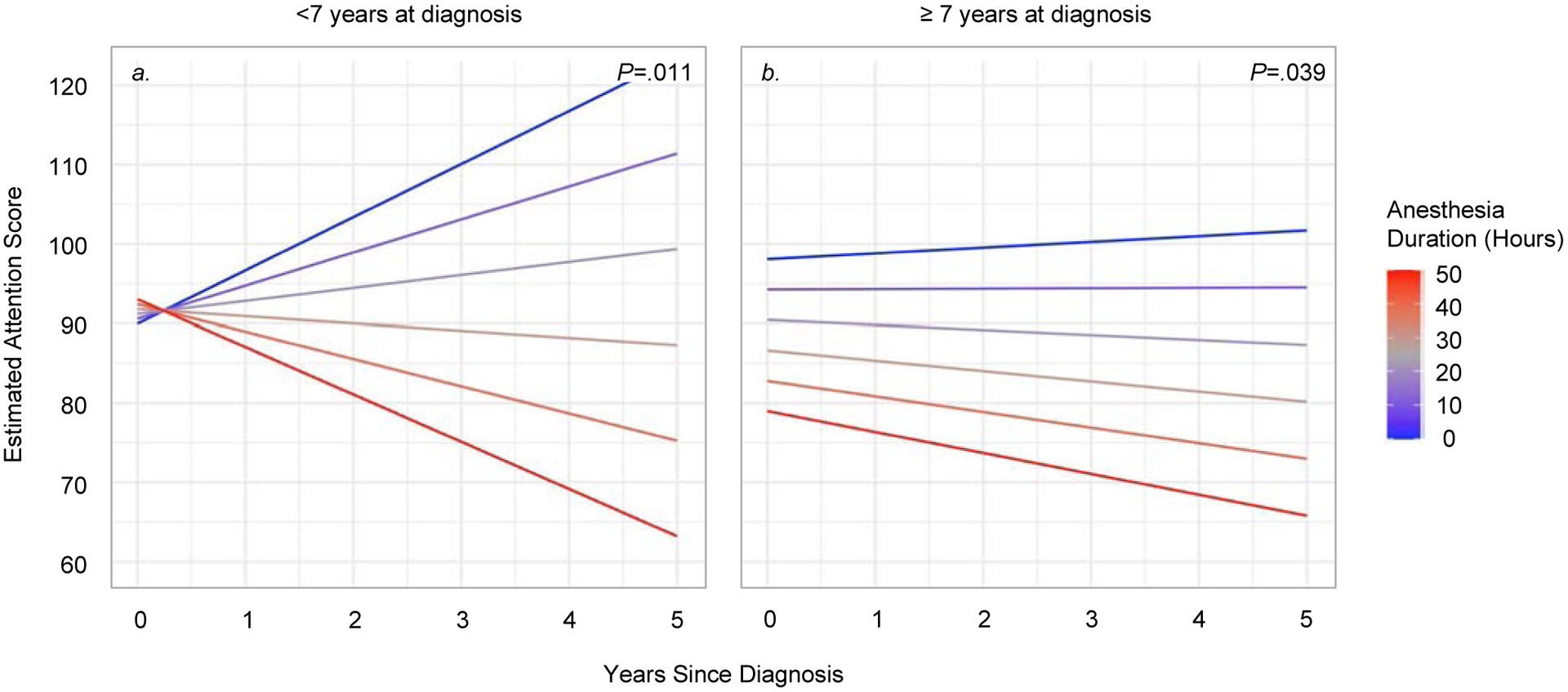
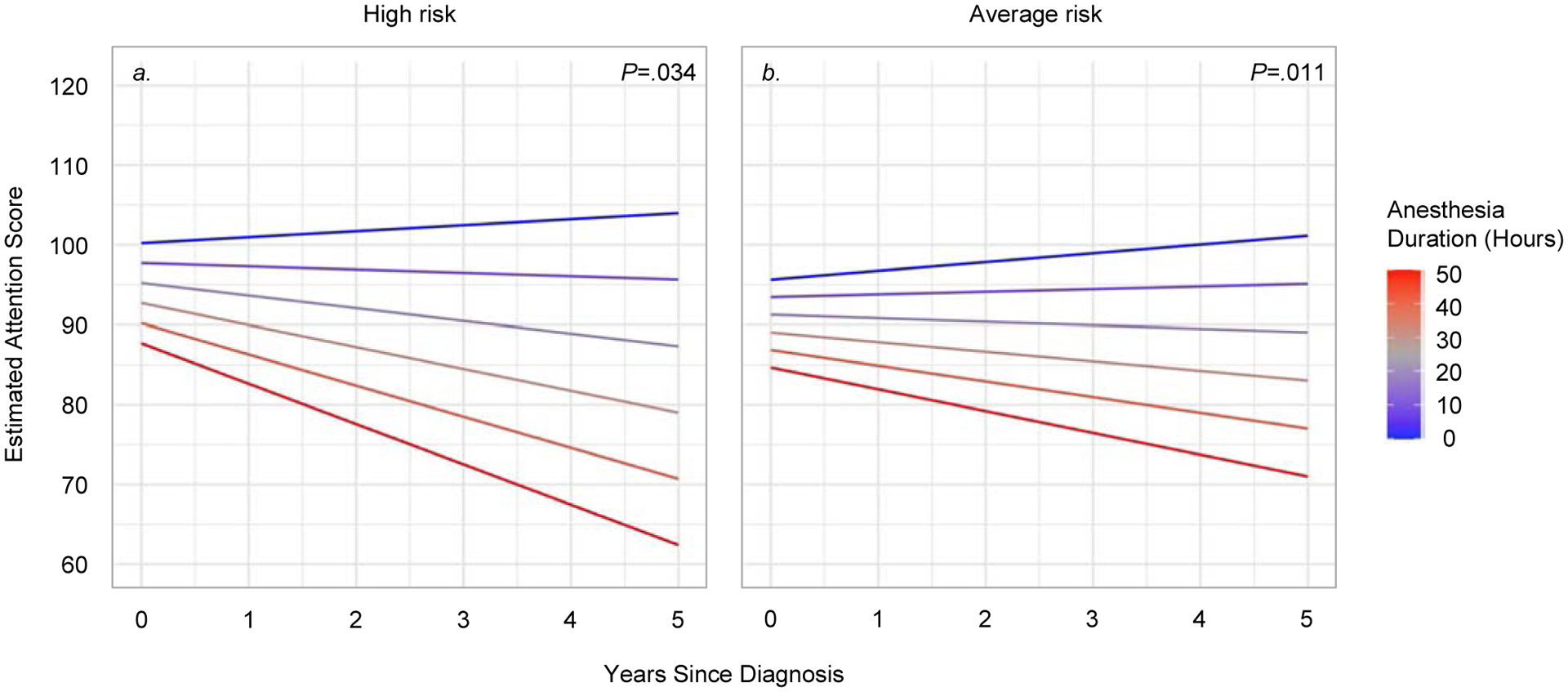
Results: Patients were 10.2 years at diagnosis on average (SD = 4.5; 37% female, 73% average-risk). Mean cumulative anesthesia duration was 20.4 h (SD = 15.2; range 0.7-55.6 h). In the overall group, longer anesthesia duration was associated with greater declines in IQ (Estimate = -0.08, P < 0.001), attention (Estimate = -0.10, P < .001) and processing speed (Estimate = -0.13, P < 0.001). Similar results were shown in subgroups of patients who were <7 years at diagnosis (IQ = -0.14, P = 0.027; Attention = -0.25: P = 0.011), ≥7 years at diagnosis (Attention = -0.07, P = 0.039; Processing Speed = -0.08, P = 0.022), treated for high-risk disease (IQ = -0.09, P = 0.024; Attention = -0.11, P = 0.034; Processing Speed = -0.13, P = 0.001), or treated for average-risk disease (IQ = -0.05, P = .022; Attention = -0.08, P = 0.011; Processing Speed = -0.10, P < 0.001).
Conclusion: Greater anesthesia exposure is a risk factor for clinically significant neurocognitive decline, in addition to factors of age at diagnosis and treatment risk arm. This result is notable as there are evidence-based strategies that can limit the need for anesthesia. Limiting anesthesia exposure, as feasible, may mitigate neurocognitive late effects, and thus, improve quality of life for survivors.
Keywords: Anesthesia; Brain tumour; Children; Longitudinal; Medulloblastoma; Neurocognitive.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Conflict of interest statement Authors have no conflicts of interest to disclose.
Figures
References
-
- Gajjar A, Chintagumpala M, Ashley D, Kellie S, Kun LE, Merchant TE, et al. Risk-adapted craniospinal radiotherapy followed by high-dose chemotherapy and stem-cell rescue in children with newly diagnosed medulloblastoma (St Jude Medulloblastoma-96): long-term results from a prospective, multicentre trial. The Lancet Oncology. 2006;7:813–20. - PubMed
-
- Robinson KE, Fraley CE, Pearson MM, Kuttesch JF, Jr., Compas BE. Neurocognitive late effects of pediatric brain tumors of the posterior fossa: a quantitative review. J Int Neuropsychol Soc. 2013;19:44–53. - PubMed
-
- Chapman CA, Waber DP, Bernstein JH, Pomeroy SL, LaVally B, Sallan SE, et al. Neurobehavioral and neurologic outcome in long-term survivors of posterior fossa brain tumors: role of age and perioperative factors. J Child Neurol. 1995;10:209–12. - PubMed
-
- Mulhern RK, Kepner JL, Thomas PR, Armstrong D, Friedman HS, Kun LE. Neuropsychologic functioning of survivors of childhood medulloblastoma randomized to receive conventional or reduced-dose craniospinal irradiation: a Pediatric Oncology Group study. J Clin Oncol. 1998;16:1723–8. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
