

Correlation between lung ultrasound and chest CT patterns with estimation of pulmonary burden in COVID-19 patients
- PMID: 33743491
- PMCID: PMC7948674
- DOI: 10.1016/j.ejrad.2021.109650
Correlation between lung ultrasound and chest CT patterns with estimation of pulmonary burden in COVID-19 patients
Abstract
Purpose: The capability of lung ultrasound (LUS) to distinguish the different pulmonary patterns of COVID-19 and quantify the disease burden compared to chest CT is still unclear.
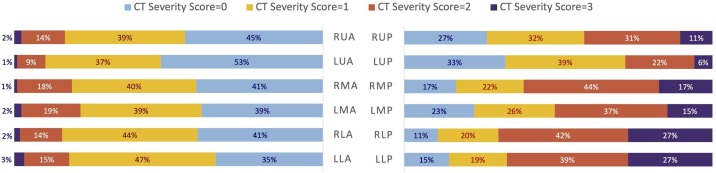
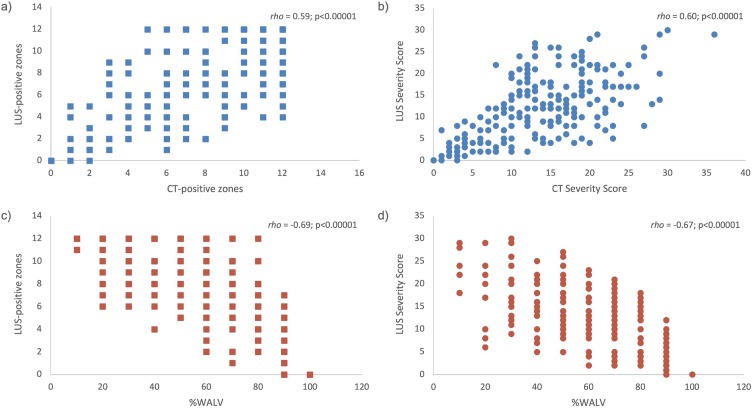
Methods: PCR-confirmed COVID-19 patients who underwent both LUS and chest CT at the Emergency Department were retrospectively analysed. In both modalities, twelve peripheral lung zones were identified and given a Severity Score basing on main lesion pattern. On CT scans the well-aerated lung volume (%WALV) was visually estimated. Per-patient and per-zone assessments of LUS classification performance taking CT findings as reference were performed, further revisioning the images in case of discordant results. Correlations between number of disease-positive lung zones, Severity Score and %WALV on both LUS and CT were assessed. The area under receiver operating characteristic curve (AUC) was calculated to determine LUS performance in detecting %WALV ≤ 70 %.
Results: The study included 219 COVID-19 patients with abnormal chest CT. LUS correctly identified as positive 217 (99 %) patients, but per-zone analysis showed sensitivity = 75 % and specificity = 66 %. The revision of the 121 (55 %) cases with positive LUS and negative CT revealed COVID-compatible lesions in 42 (38 %) CT scans. Number of disease-positive zones, Severity Score and %WALV between LUS and CT showed moderate correlations. The AUCs for LUS Severity Score and number of LUS-positive zones did not differ in detecting %WALV ≤ 70 %.
Conclusion: LUS in COVID-19 is valuable for case identification but shows only moderate correlation with CT findings as for lesion patterns and severity quantification. The number of disease-positive lung zones in LUS alone was sufficient to discriminate relevant disease burden.
Keywords: COVID-19; Diagnostic techniques and procedures; Lung; Tomography; Ultrasonography; X-Ray computed.
Copyright © 2021 Elsevier B.V. All rights reserved.
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article.
Figures





References
-
- World Health Organization . 2020. Novel Coronavirus (2019-nCoV) Situation Report - 11.https://www.who.int/docs/default-source/coronaviruse/situation-reports/2... Geneva (Switzerland)
-
- World Health Organization . 2020. Coronavirus Disease 2019 (COVID-19) Situation Report – 51.https://www.who.int/docs/default-source/coronaviruse/situation-reports/2... Geneva (Switzerland)
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
