

Opioid-induced respiratory depression increases hospital costs and length of stay in patients recovering on the general care floor
- PMID: 33743588
- PMCID: PMC7980593
- DOI: 10.1186/s12871-021-01307-8
Opioid-induced respiratory depression increases hospital costs and length of stay in patients recovering on the general care floor
Abstract
Background: Opioid-induced respiratory depression is common on the general care floor. However, the clinical and economic burden of respiratory depression is not well-described. The PRediction of Opioid-induced respiratory Depression In patients monitored by capnoGraphY (PRODIGY) trial created a prediction tool to identify patients at risk of respiratory depression. The purpose of this retrospective sub-analysis was to examine healthcare utilization and hospital cost associated with respiratory depression.
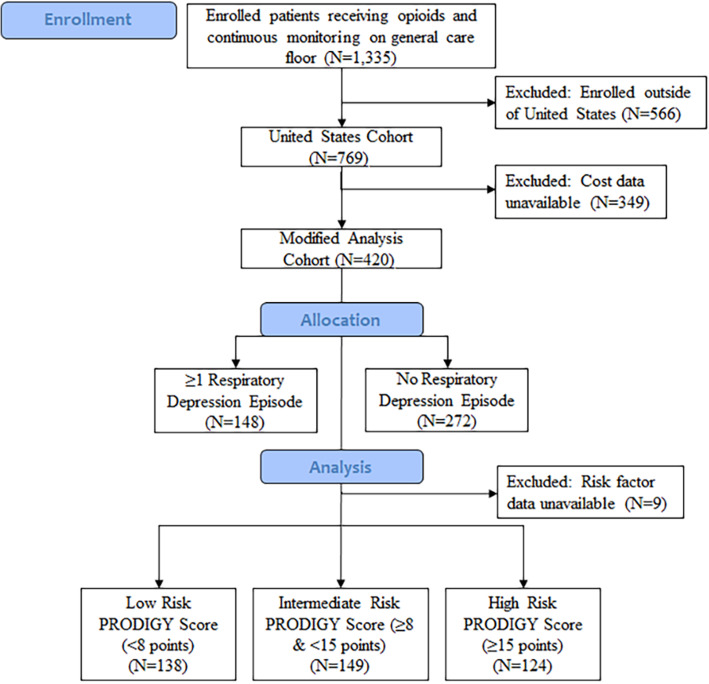
Methods: One thousand three hundred thirty-five patients (N = 769 United States patients) enrolled in the PRODIGY trial received parenteral opioids and underwent continuous capnography and pulse oximetry monitoring. Cost data was retrospectively collected for 420 United States patients. Differences in healthcare utilization and costs between patients with and without ≥1 respiratory depression episode were determined. The impact of respiratory depression on hospital cost per patient was evaluated using a propensity weighted generalized linear model.
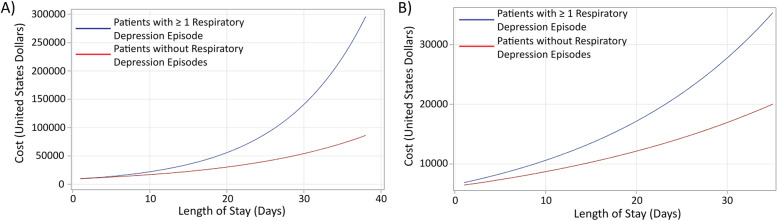
Results: Patients with ≥1 respiratory depression episode had a longer length of stay (6.4 ± 7.8 days vs 5.0 ± 4.3 days, p = 0.009) and higher hospital cost ($21,892 ± $11,540 vs $18,206 ± $10,864, p = 0.002) compared to patients without respiratory depression. Patients at high risk for respiratory depression, determined using the PRODIGY risk prediction tool, who had ≥1 respiratory depression episode had higher hospital costs compared to high risk patients without respiratory depression ($21,948 ± $9128 vs $18,474 ± $9767, p = 0.0495). Propensity weighted analysis identified 17% higher costs for patients with ≥1 respiratory depression episode (p = 0.007). Length of stay significantly increased total cost, with cost increasing exponentially for patients with ≥1 respiratory depression episode as length of stay increased.
Conclusions: Respiratory depression on the general care floor is associated with a significantly longer length of stay and increased hospital costs. Early identification of patients at risk for respiratory depression, along with early proactive intervention, may reduce the incidence of respiratory depression and its associated clinical and economic burden.
Trial registration: ClinicalTrials.gov , NCT02811302 .
Keywords: Costs; Detection; Healthcare utilization; Monitoring; Opioids; Patient safety; Post-operative; Respiratory depression.
Conflict of interest statement
All authors (or their institutions) received research support from Medtronic to conduct this trial.
In addition, AK reports consulting fees from Medtronic, Edwards Lifesciences, and Philips North America, AK is supported by an NIH/NCATS Wake Forest CTSI award for a randomized trial of continuous postoperative hemodynamic and respiratory monitoring; LS reports a grant from Merck & Co. Inc. and consultant fees from Merck & Co. Inc., The 37 Company, and Ferrer International; CRJ reports participation in the Medtronic Nurse Advisory Group; SU reports speaker honorarium from Edwards Lifescience, LTD; WJ reports receiving a salary from Medtronic; WB reports grants from the European Union and Interreg Consortium, and personal fees from European Society of Anaesthesiology studies (PHOENICS and TETHYS) supported by B Braun Medical and Fresenius Medical Care, and from Medtronic.
Figures
References
-
- Andersen LW, Berg KM, Chase M, Cocchi MN, Massaro J, Donnino MW, American Heart Association's get with the guidelines-resuscitation I Acute respiratory compromise on inpatient wards in the United States: incidence, outcomes, and factors associated with in-hospital mortality. Resuscitation. 2016;105:123–129. doi: 10.1016/j.resuscitation.2016.05.014. - DOI - PubMed
-
- Pearse RM, Moreno RP, Bauer P, Pelosi P, Metnitz P, Spies C, Vallet B, Vincent JL, Hoeft A, Rhodes A, European Surgical Outcomes Study (EuSOS) group for the Trials groups of the European Society of Intensive Care Medicine and the European Society of Anaesthesiology Mortality after surgery in Europe: a 7 day cohort study. Lancet. 2012;380(9847):1059–1065. doi: 10.1016/S0140-6736(12)61148-9. - DOI - PMC - PubMed
-
- Khanna AK, Bergese SD, Jungquist CR, Morimatsu H, Uezono S, Lee S, Ti LK, Urman RD, McIntyre R, Jr, Tornero C, et al. Prediction of opioid-induced respiratory depression on inpatient wards using continuous Capnography and Oximetry: an international prospective, Observational Trial. Anesth Analg. 2020;131(4):1012–1024. doi: 10.1213/ANE.0000000000004788. - DOI - PMC - PubMed
-
- Sun Z, Sessler DI, Dalton JE, Devereaux PJ, Shahinyan A, Naylor AJ, Hutcherson MT, Finnegan PS, Tandon V, Darvish-Kazem S, Chugh S, Alzayer H, Kurz A. Postoperative hypoxemia is common and persistent: a prospective blinded observational study. Anesth Analg. 2015;121(3):709–715. doi: 10.1213/ANE.0000000000000836. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
