

A 78-year-old female with severe tongue pain: benefit of modern ultrasound
- PMID: 33743613
- PMCID: PMC7981810
- DOI: 10.1186/s12880-021-00585-5
A 78-year-old female with severe tongue pain: benefit of modern ultrasound
Abstract
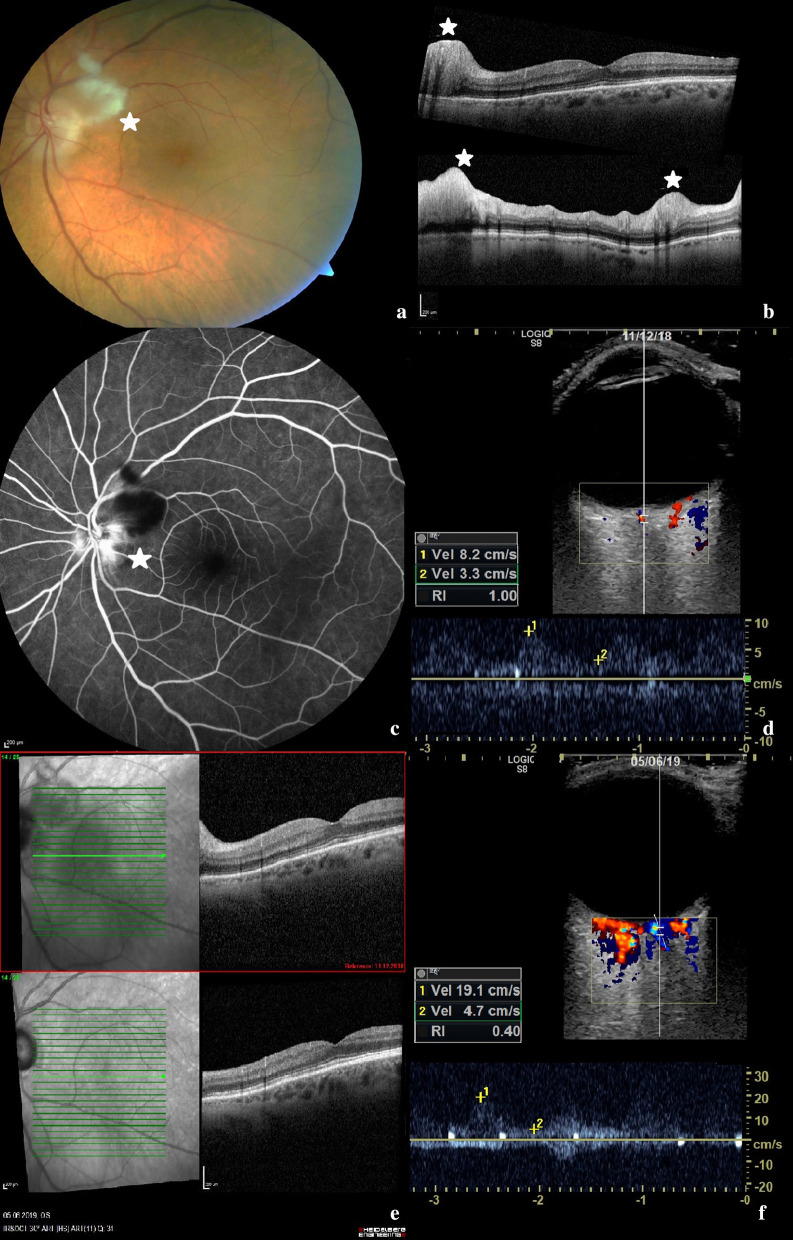
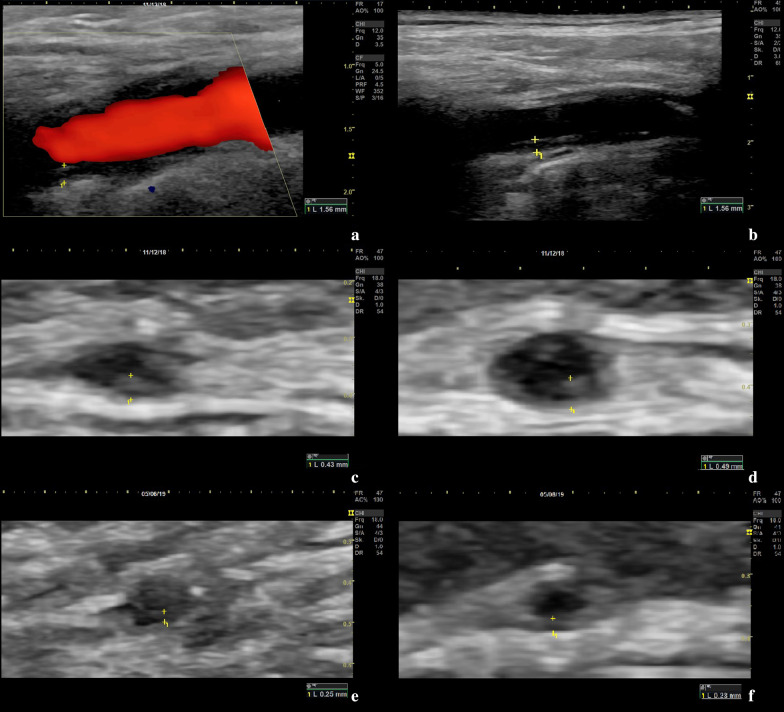
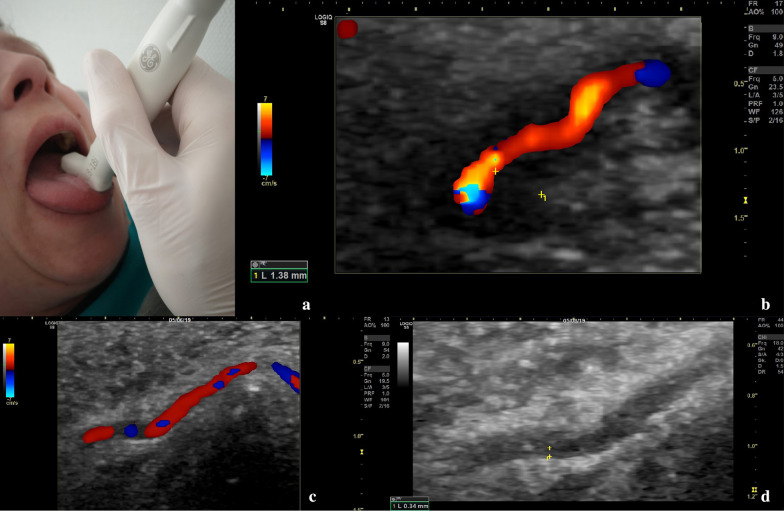
Background: Giant cell arteritis (GCA) is the most common form of systemic vasculitis in persons aged 50 years and older. Medium and large vessels, like the temporal and axillary arteries, are commonly affected. Typical symptoms are headache, scalp tenderness, jaw claudication and ophthalmological symptoms as loss of visual field, diplopia or amaurosis due to optic nerve ischemia. Tongue pain due to vasculitic affection of the deep lingual artery can occur and has so far not been visualized and followed up by modern ultrasound.
Case presentation: We report the case of a 78-year-old woman with typical symptoms of GCA, such as scalp tenderness, jaw claudication and loss of visual field, as well as severe tongue pain. Broad vasculitic affection of the extracranial arteries, vasculitis of the central retinal artery and the deep lingual artery could be visualized by ultrasound. Further did we observe a relevant decrease of intima-media thickness (IMT) values of all arteries assessed by ultrasound during follow-up. Especially the left common superficial temporal artery showed a relevant decrease of IMT from 0.49 mm at time of diagnosis to 0.23 mm on 6-months follow-up. This is the first GCA case described in literature, in which vasculitis of the central retinal artery and the lingual artery could be visualized at diagnosis and during follow-up using high-resolution ultrasound.
Conclusion: High-resolution ultrasound can be a useful diagnostic imaging modality in diagnosis and follow-up of GCA, even in small arteries like the lingual artery or central retinal artery. Ultrasound of the central retinal artery could be an important imaging tool in identifying suspected vasculitic affection of the central retinal artery.
Keywords: Central retinal artery; Follow-up; Giant cell arteritis; Intima-media thickness; Lingual artery; Ultrasound; Vasculitis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Warrington KJ, Matteson EL. Management guidelines and outcome measures in giant cell arteritis (GCA) Clin Exp Rheumatol. 2007;25:137–141. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
