

The technical feasibility and preliminary results of minimally invasive endoscopic-TLIF based on electromagnetic navigation: a case series
- PMID: 33743668
- PMCID: PMC7981827
- DOI: 10.1186/s12893-021-01148-9
The technical feasibility and preliminary results of minimally invasive endoscopic-TLIF based on electromagnetic navigation: a case series
Abstract
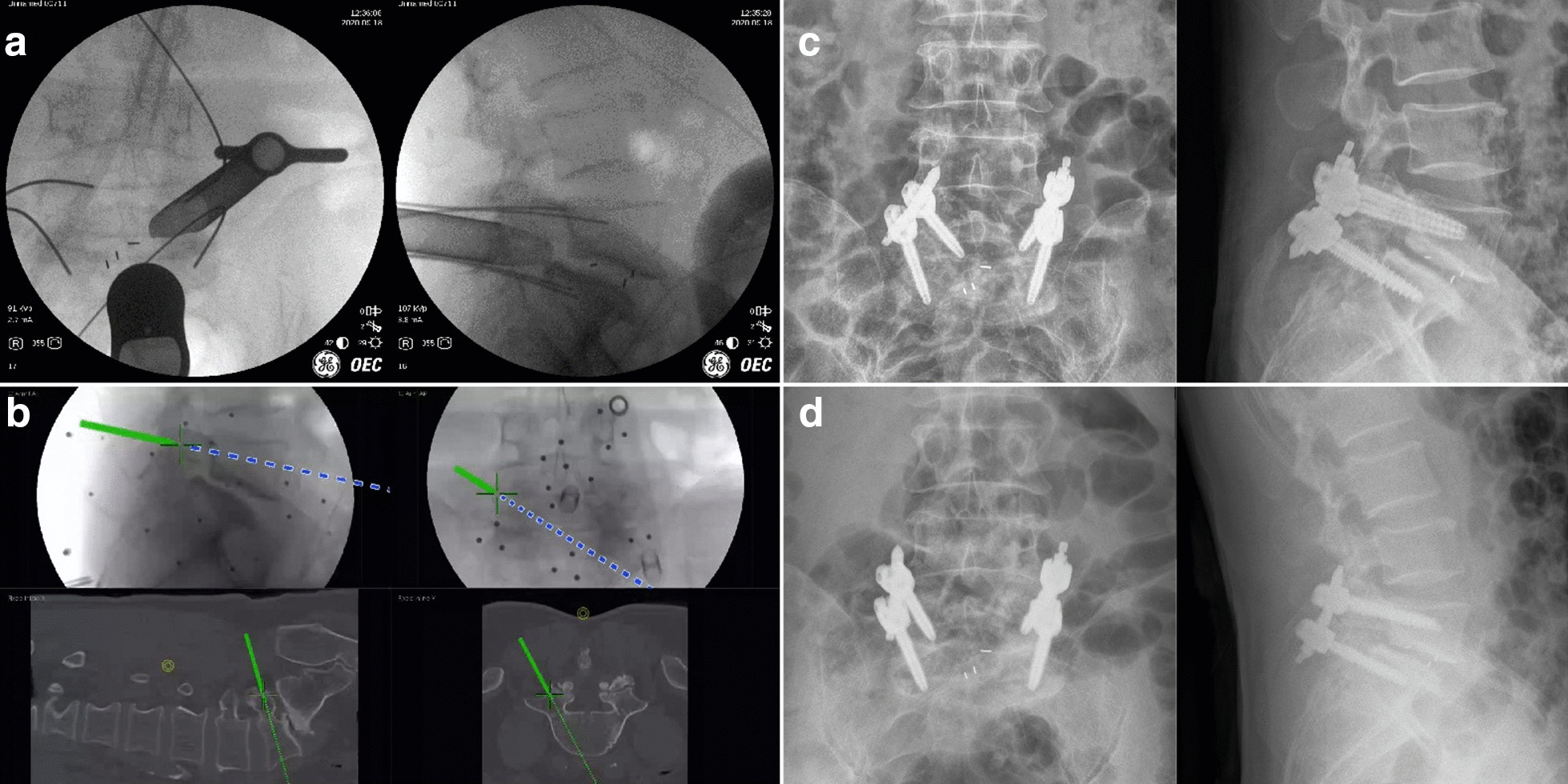
Background: Uniportal full endoscopic posterolateral transforaminal lumbar interbody fusion (Endo-TLIF) with percutaneous pedicle screw fixation is a promising, minimally invasive method for the treatment of lumbar spondylolisthesis. However, repeated radiation exposure from X-rays and the steep learning curve remain to be improved.
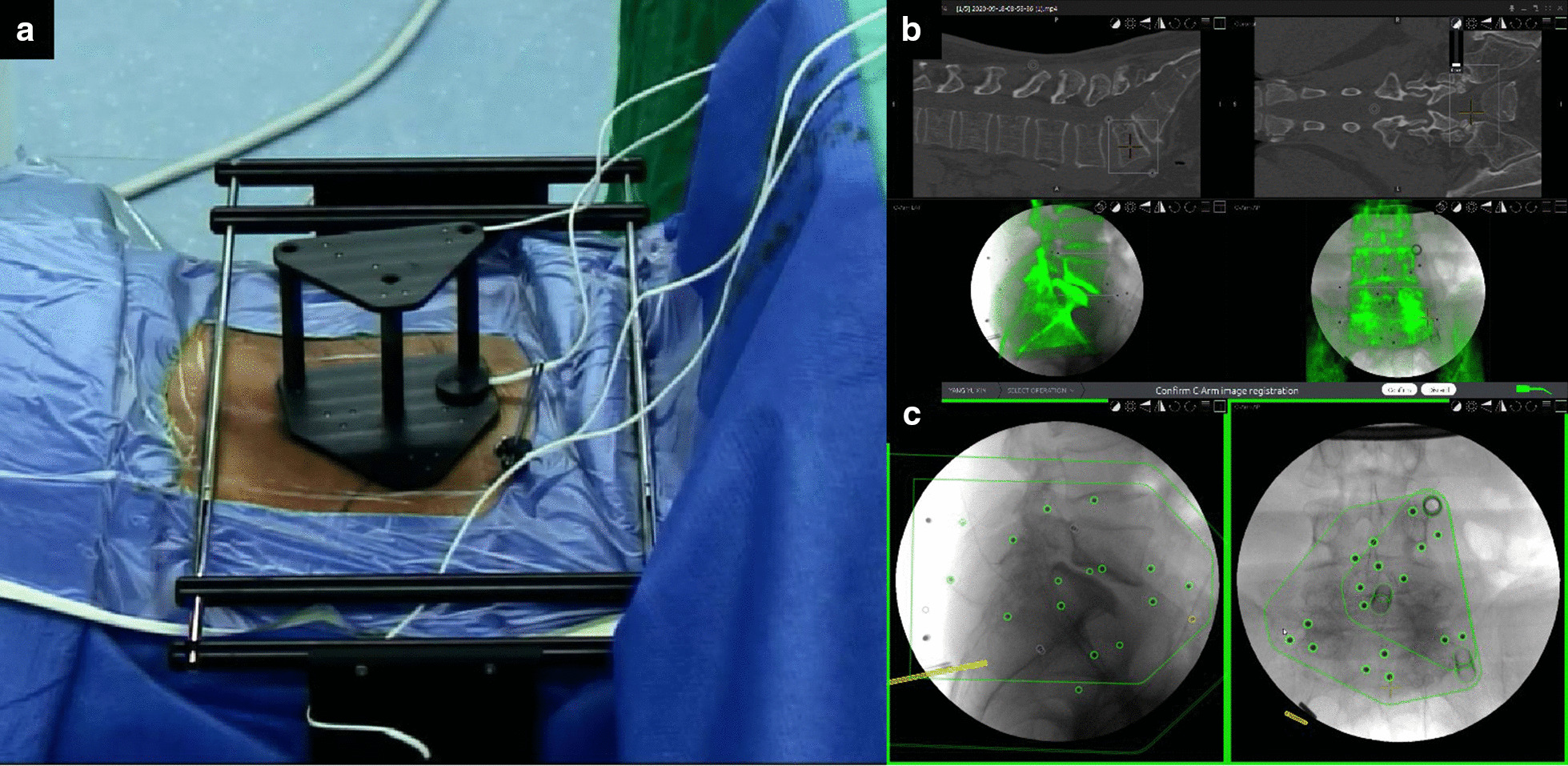
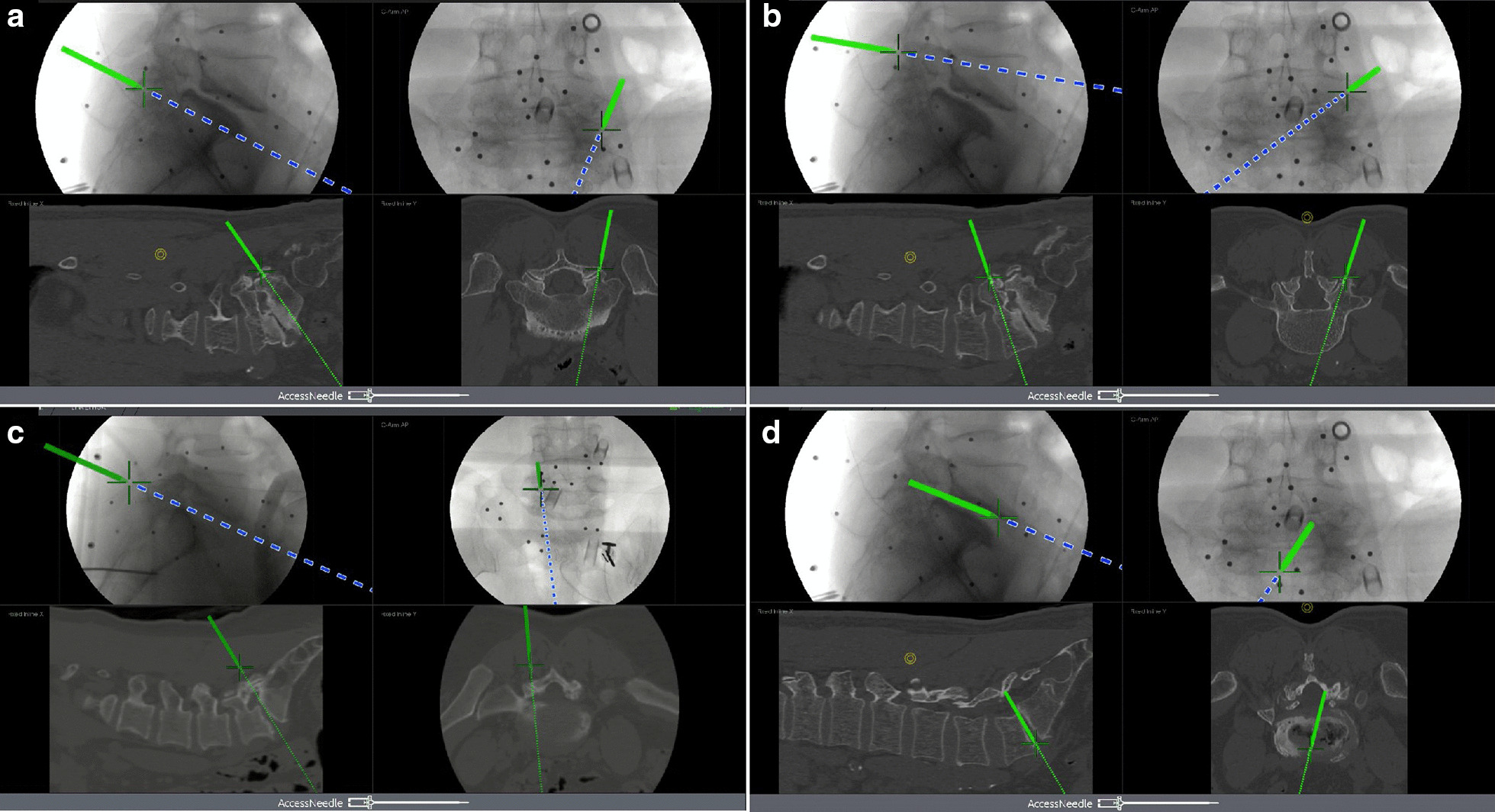
Methods: This retrospective study explored the effects of electromagnetic navigation on improving Endo-TLIF with percutaneous pedicle screw fixation. Clinical information from 42 patients who had received Endo-TLIF with percutaneous pedicle screw fixation from May 2019 to November 2020 was analyzed retrospectively. The procedures were assisted under electromagnetic navigation. The rate of adjustment for guide wires, frequency of X-ray exposure, operative time, accuracy of pedicle screw location, and clinical outcomes were recorded.
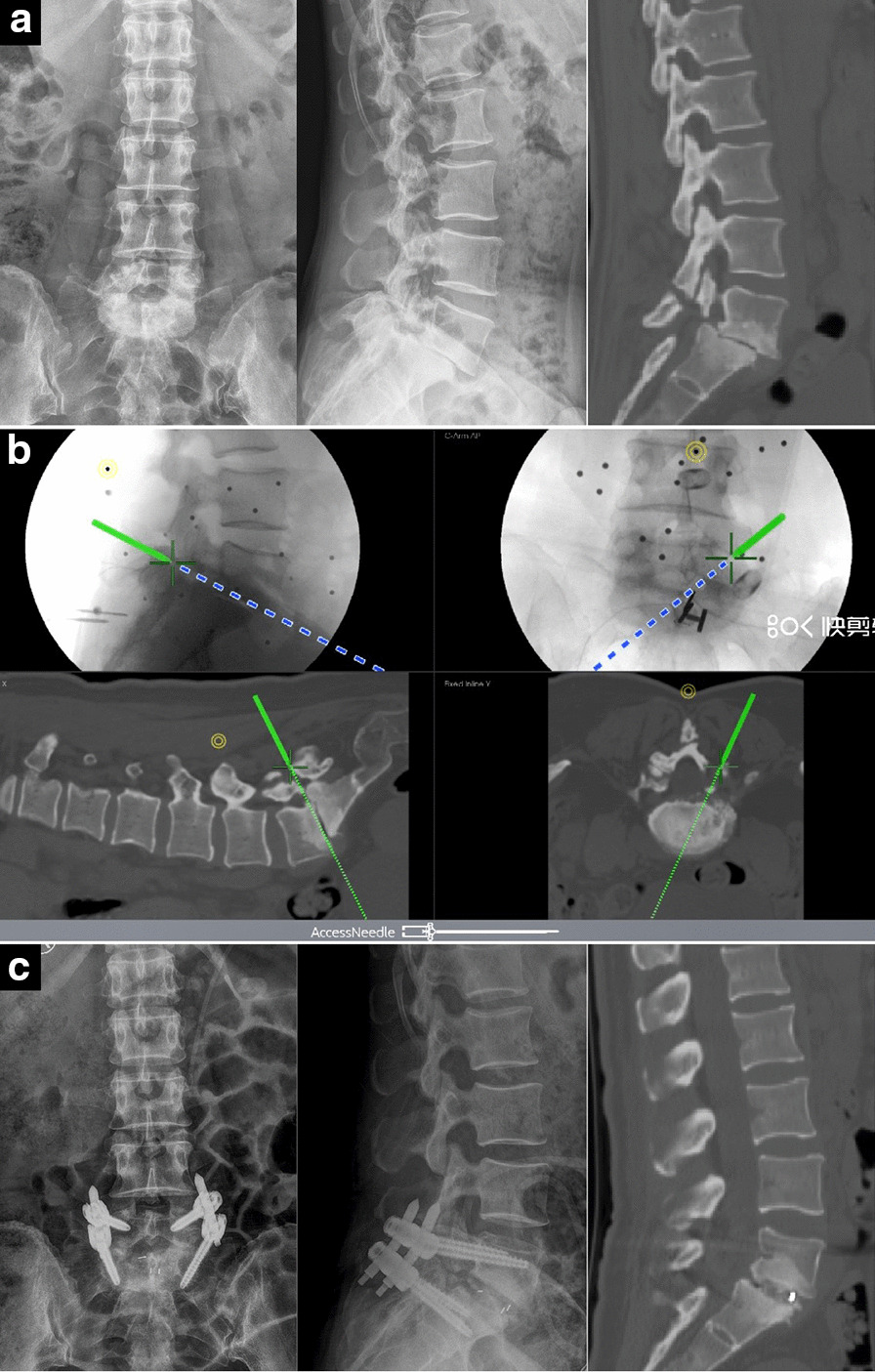
Results: The mean follow-up for 42 patients was 11.9 ± 3.1 months. The mean age of the patients was 56.1 ± 9.26 years, with a female/male ratio of 25:17. According to postoperative CT scans and 3D reconstructions, the excellent and good rate of pedicle screws was 96.4%. The rate of adjustment for guide wires under the assistance of electromagnetic navigation was 1.78%, and the frequency of X-ray exposure was 8.27 ± 1.83. The operative time was 167.25 ± 28.16 min, including the duration of guide wire insertion (14.63 ± 5.45 min) and duration of decompression and cage placement (75.43 ± 13.97 min). The duration of hospitalization after operation was 2.59 ± 1.16 days. The preoperative VAS score was 7.51 ± 1.91, and the preoperative ODI was 82.42 ± 8.7%. At the last follow-up, the VAS score was 2.09 ± 0.59, and the ODI was 11.09 ± 3.2%. There were statistically significant improvements in the VAS score and ODI in all patients at the follow-up (p < 0.05).
Conclusions: Electromagnetic navigation can provide accurate positioning and guidance in real time, which improves the surgical efficiency of percutaneous pedicle screw placement and endoscopic decompression in Endo-TLIF with reduced radiation exposures.
Keywords: Electromagnetic navigation; Endo-TLIF; Lumbar spondylolisthesis; Percutaneous pedicle screw.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
Similar articles
-
Comparison of electromagnetic and optical navigation assisted Endo-TLIF in the treatment of lumbar spondylolisthesis.BMC Musculoskelet Disord. 2022 Jun 1;23(1):522. doi: 10.1186/s12891-022-05443-1. BMC Musculoskelet Disord. 2022. PMID: 35650587 Free PMC article.
-
Early Clinical Evaluation of Percutaneous Full-endoscopic Transforaminal Lumbar Interbody Fusion with Pedicle Screw Insertion for Treating Degenerative Lumbar Spinal Stenosis.Orthop Surg. 2021 Feb;13(1):328-337. doi: 10.1111/os.12900. Epub 2021 Jan 10. Orthop Surg. 2021. PMID: 33426744 Free PMC article.
-
Percutaneous Endoscopic Robot-Assisted Transforaminal Lumbar Interbody Fusion (PE RA-TLIF) for Lumbar Spondylolisthesis: A Technical Note and Two Years Clinical Results.Pain Physician. 2022 Jan;25(1):E73-E86. Pain Physician. 2022. PMID: 35051154
-
Clinical Results and Complications of Endoscopic Lumbar Interbody Fusion for Lumbar Degenerative Disease: A Meta-Analysis.World Neurosurg. 2021 Jan;145:396-404. doi: 10.1016/j.wneu.2020.10.033. Epub 2020 Oct 13. World Neurosurg. 2021. PMID: 33065349 Review.
-
Minimally Invasive Transforaminal Lumbar Interbody Fusion with Percutaneous Bilateral Pedicle Screw Fixation for Lumbosacral Spine Degenerative Diseases. A Retrospective Database of 40 Consecutive Cases and Literature Review.Turk Neurosurg. 2018;28(3):454-461. doi: 10.5137/1019-5149.JTN.19479-16.0. Turk Neurosurg. 2018. PMID: 28481388 Review.
Cited by
-
Navigation Techniques in Endoscopic Spine Surgery.Biomed Res Int. 2022 Aug 29;2022:8419739. doi: 10.1155/2022/8419739. eCollection 2022. Biomed Res Int. 2022. PMID: 36072476 Free PMC article. Review.
-
Determining the learning curve for percutaneous endoscopic lumbar interbody fusion for lumbar degenerative diseases.J Orthop Surg Res. 2023 Mar 12;18(1):193. doi: 10.1186/s13018-023-03682-z. J Orthop Surg Res. 2023. PMID: 36907913 Free PMC article.
-
The Utilization of Navigation and Emerging Technologies With Endoscopic Spine Surgery: A Narrative Review.Neurospine. 2025 Mar;22(1):105-117. doi: 10.14245/ns.2449404.702. Epub 2025 Mar 31. Neurospine. 2025. PMID: 40211520 Free PMC article.
-
Comprehensive workflow with optical navigation in minimally invasive transforaminal lumbar interbody fusion: a retrospective study.J Orthop Surg Res. 2025 Jul 21;20(1):694. doi: 10.1186/s13018-025-06111-5. J Orthop Surg Res. 2025. PMID: 40691597 Free PMC article. Review.
-
Fully Endoscopic 360° Decompression for Central Lumbar Spinal Stenosis Combined with Disc Herniation: Technical Note and Preliminary Outcomes of 39 Cases.J Pain Res. 2022 Sep 13;15:2867-2878. doi: 10.2147/JPR.S379431. eCollection 2022. J Pain Res. 2022. PMID: 36124038 Free PMC article.
References
-
- Glassman SD, Carreon LY, Ghogawala Z, et al. Benefit of transforaminal lumbar interbody fusion vs posterolateral spinal fusion in lumbar spine disorders: a propensity-matched analysis from the national neurosurgical quality and outcomes database registry. Neurosurgery. 2016;79(3):397–405. doi: 10.1227/NEU.0000000000001118. - DOI - PubMed
-
- Millimaggi DF, Norcia VD, Luzzi S, et al. Minimally invasive transforaminal lumbar interbody fusion with percutaneous bilateral pedicle screw fixation for lumbosacral spine degenerative diseases. A retrospective database of 40 consecutive cases and literature review. Turk Neurosurg. 2018;28(3):454–461. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
