

Mechanical ventilation parameters in critically ill COVID-19 patients: a scoping review
- PMID: 33743812
- PMCID: PMC7980724
- DOI: 10.1186/s13054-021-03536-2
Mechanical ventilation parameters in critically ill COVID-19 patients: a scoping review
Abstract
Background: The mortality of critically ill patients with COVID-19 is high, particularly among those receiving mechanical ventilation (MV). Despite the high number of patients treated worldwide, data on respiratory mechanics are currently scarce and the optimal setting of MV remains to be defined. This scoping review aims to provide an overview of available data about respiratory mechanics, gas exchange and MV settings in patients admitted to intensive care units (ICUs) for COVID-19-associated acute respiratory failure, and to identify knowledge gaps.
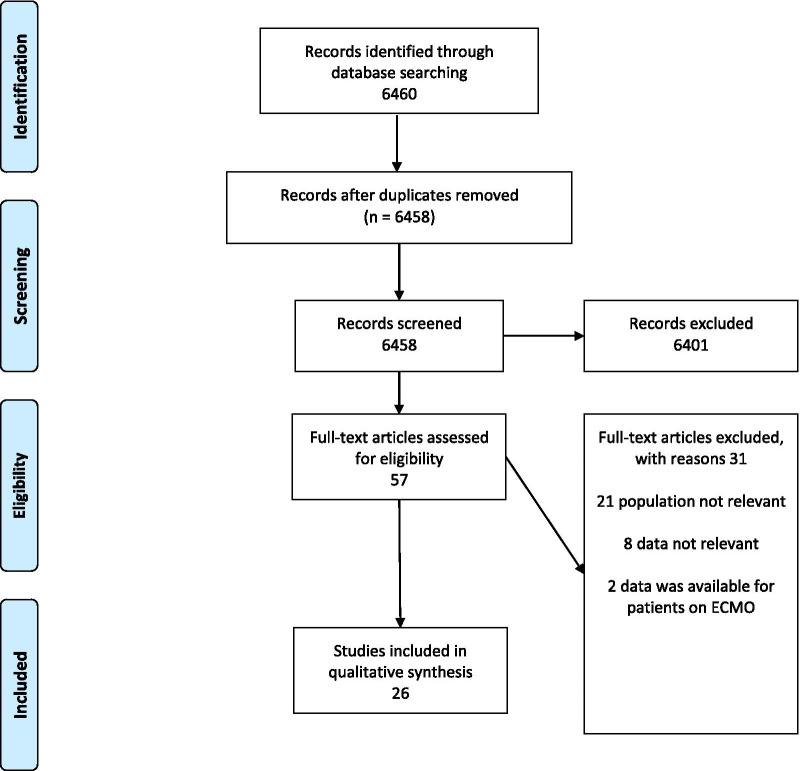
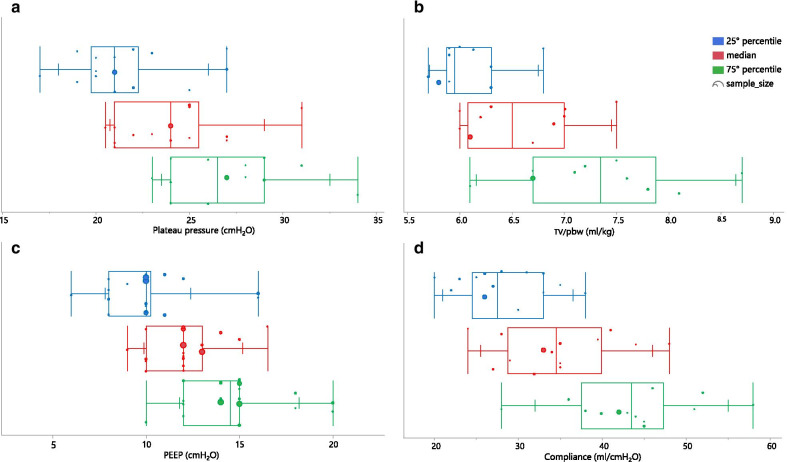
Main text: PubMed, EMBASE, and MEDLINE databases were searched from inception to October 30, 2020 for studies providing at least one ventilatory parameter collected within 24 h from the ICU admission. The quality of the studies was independently assessed using the Newcastle-Ottawa Quality Assessment Form for Cohort Studies. A total of 26 studies were included for a total of 14,075 patients. At ICU admission, positive end expiratory pressure (PEEP) values ranged from 9 to 16.5 cm of water (cmH2O), suggesting that high levels of PEEP were commonly used for setting MV for these patients. Patients with COVID-19 are severely hypoxemic at ICU admission and show a median ratio of partial pressure of arterial oxygen to fraction of inspired oxygen (PaO2/FiO2) ranging from 102 to 198 mmHg. Static respiratory system compliance (Crs) values at ICU admission were highly heterogenous, ranging between 24 and 49 ml/cmH2O. Prone positioning and neuromuscular blocking agents were widely used, ranging from 17 to 81 and 22 to 88%, respectively; both rates were higher than previously reported in patients with "classical" acute respiratory distress syndrome (ARDS).
Conclusions: Available data show that, in mechanically ventilated patients with COVID-19, respiratory mechanics and MV settings within 24 h from ICU admission are heterogeneous but similar to those reported for "classical" ARDS. However, to date, complete data regarding mechanical properties of respiratory system, optimal setting of MV and the role of rescue treatments for refractory hypoxemia are still lacking in the medical literature.
Keywords: Acute respiratory distress syndrome; Coronavirus disease 2019; Intensive care units; Mechanical ventilation.
Conflict of interest statement
Dr. Grasselli reports personal fees from Maquet, personal fees from Biotest, personal fees from Pfizer, personal fees from Draeger, personal fees from Fisher&Paykel, personal fees from MSD. Dr. Zanella has patent ES2732104 licensed to AW Technologies and patents US2017348472 and US2017224898 licensed to Fresenius. Dr. Pesenti reports personal fees from Maquet, Novalung/Xenios, Baxter, and Boehringer Ingelheim. Dr. Einav has support from Zoll, Siemens and Medtronic, research funding from Oridion, Diasorin, Haemonetics, participation in multicenter trials for Artisanpharma, Ely Lily, Takeda, Astra Zeneca, Eisai. The other authors declare that they have no competing interests.
Figures
References
-
- World Health Organisation. Coronavirus disease (COVID-19) Weekly epidemiological update and weekly operational update. Weekly epidemiological update Published 20 October 2020. Available at: https://www.who.int/docs/default-source/coronaviruse/situation-re.
-
- CDC, COVID-19 Pandemic Planning Scenarios. https://www.cdc.gov/coronavirus/2019-ncov/hcp/planning-scenarios.html#ta.... Accessed 16 Dec 2020.
-
- CDC Cases, Data, and Surveillance. Available at https://protect-public.hhs.gov/pages/hospital-capacity. Accessed 16 Dec 2020.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
