

Ischemia-Mediated Dysfunction in Subpapillary Myocardium as a Marker of Functional Mitral Regurgitation
- PMID: 33744130
- PMCID: PMC8086776
- DOI: 10.1016/j.jcmg.2021.01.007
Ischemia-Mediated Dysfunction in Subpapillary Myocardium as a Marker of Functional Mitral Regurgitation
Abstract
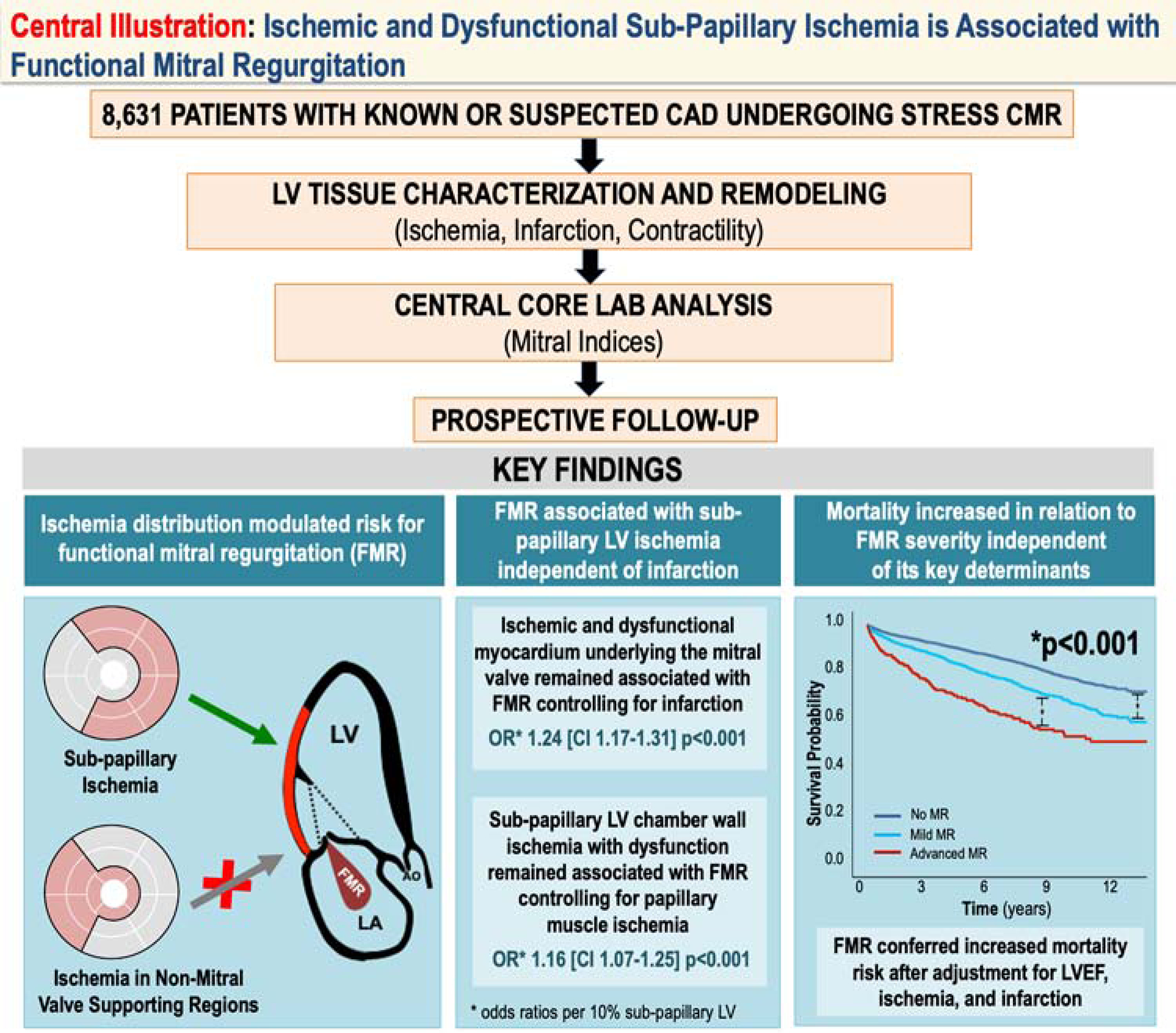
Objectives: The goal of this study was to test whether ischemia-mediated contractile dysfunction underlying the mitral valve affects functional mitral regurgitation (FMR) and the prognostic impact of FMR.
Background: FMR results from left ventricular (LV) remodeling, which can stem from myocardial tissue alterations. Stress cardiac magnetic resonance can assess ischemia and infarction in the left ventricle and papillary muscles; relative impact on FMR is uncertain.
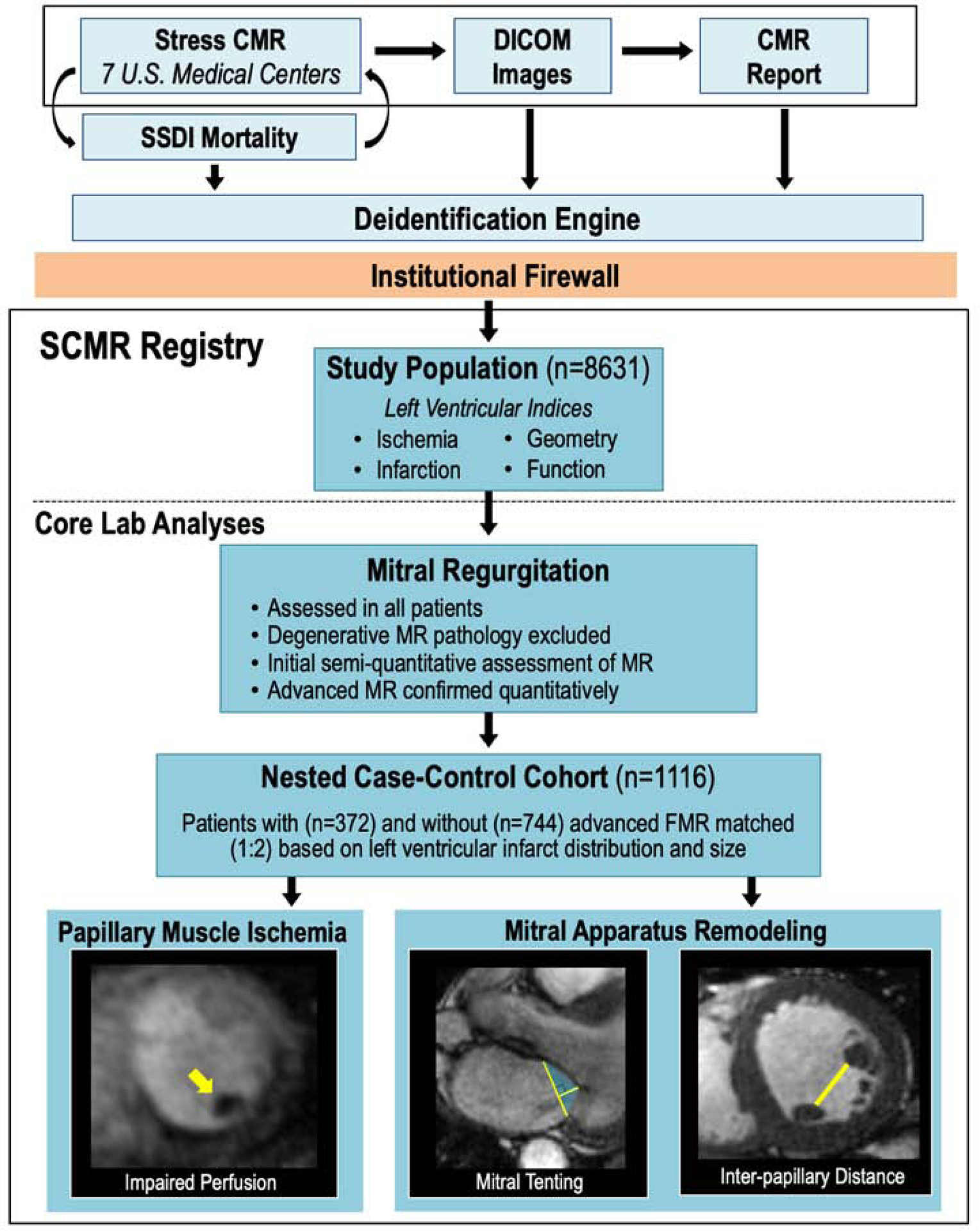
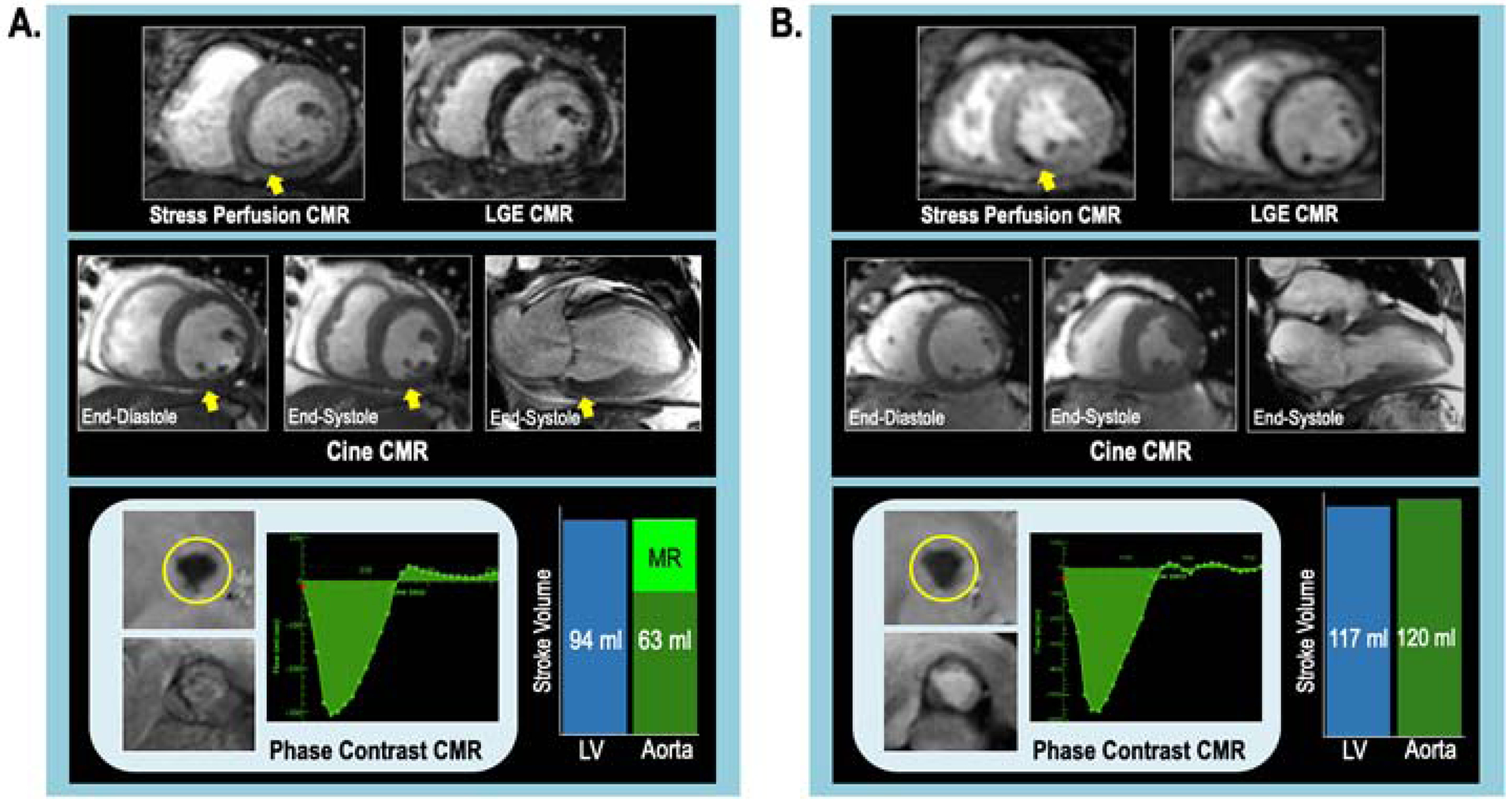
Methods: Vasodilator stress cardiac magnetic resonance was performed in patients with known or suspected coronary artery disease at 7 sites. Images were centrally analyzed for MR etiology/severity, mitral apparatus remodeling, and papillary ischemia.
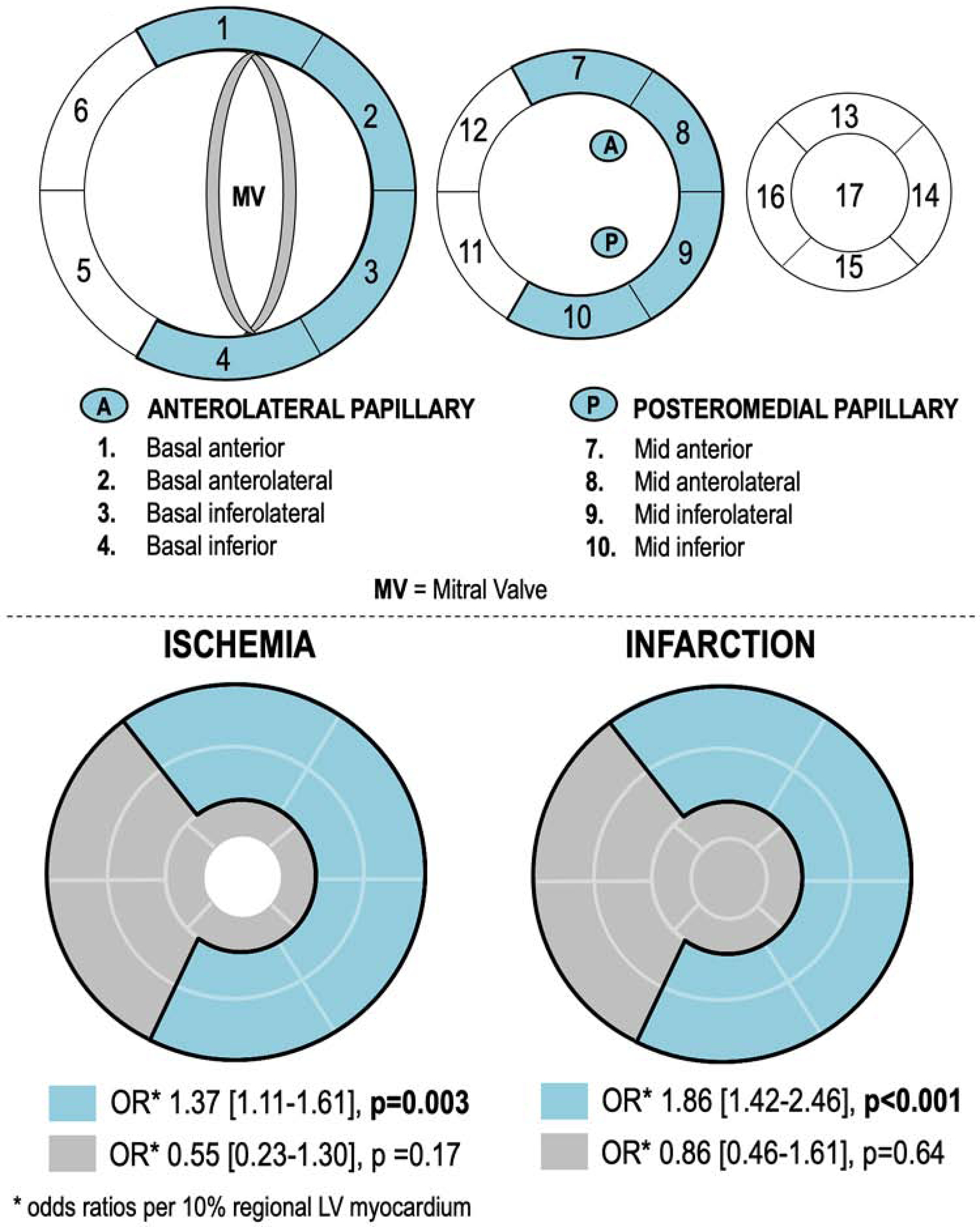
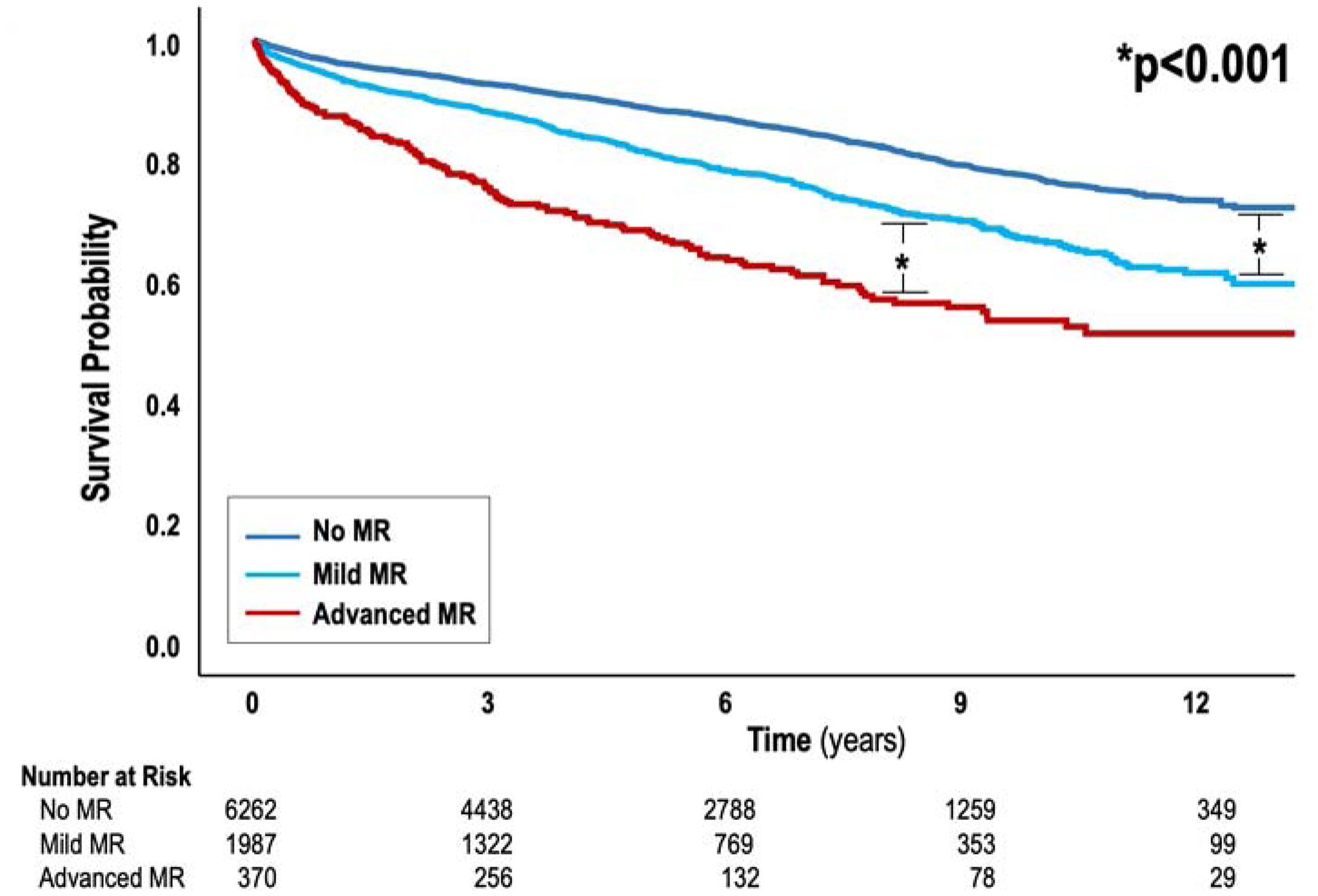
Results: A total of 8,631 patients (mean age 60.0 ± 14.1 years; 55% male) were studied. FMR was present in 27%, among whom 16% (n = 372) had advanced (moderate or severe) FMR. Patients with ischemia localized to subpapillary regions were more likely to have advanced FMR (p = 0.003); those with ischemia localized to other areas were not (p = 0.17). Ischemic/dysfunctional subpapillary myocardium (odds ratio: 1.24/10% subpapillary myocardium; confidence interval: 1.17 to 1.31; p < 0.001) was associated with advanced FMR controlling for infarction. Among a subgroup with (n = 372) and without (n = 744) advanced FMR matched (1:2) on infarct size/distribution, patients with advanced FMR had increased adverse mitral apparatus remodeling, paralleled by greater ischemic/dysfunctional subpapillary myocardium (p < 0.001). Although posteromedial papillary ischemia was more common with advanced FMR (p = 0.006), subpapillary ischemia with dysfunction remained associated (p < 0.001), adjusting for posteromedial papillary ischemia (p = 0.074). During follow-up (median 5.1 years), 1,473 deaths occurred in the overall cohort; advanced FMR conferred increased mortality risk (hazard ratio: 1.52; 95% confidence interval: 1.25 to 1.86; p < 0.001) controlling for left ventricular ejection fraction, infarction, and ischemia.
Conclusions: Ischemic and dysfunctional subpapillary myocardium provides a substrate for FMR, which predicts mortality independent of key mechanistic substrates.
Keywords: cardiac magnetic resonance; ischemia; mitral regurgitation.
Copyright © 2021 American College of Cardiology Foundation. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures This study was supported by the National Institutes of Health grants R01 HL128278 (Drs. Weinsaft, Ratcliffe, Levine, and J. Kim), R01 HL128099 and R01 HL141917 (Dr. Levine), R01-HL63348 (Dr. Ratcliffe), K23 HL140092 (Dr. J. Kim), K23 HL132011 (Dr. Shenoy), and T32 HL7854-23 (Dr. Kochav). It was also funded by the Glorney-Raisbeck Fellowship/NY Academy of Medicine (Dr. Kochav). Dr. Judd has an equity interest. Dr. R. Kim serves on the Board of Directors. Mr. Cargile is an employee of Heart Imaging Technologies. Dr. Klem is a consultant for and receives speaker honorarium from Bayer; and receives funding from Medtronic. Dr. Karmpaliotis receives funding from Abbott Vascular, Boston Scientific, and Abiomed; and has equity in Saranas, Soundbite, and Traverse Vascular. Dr. Leon receives funding from Abbott Vascular, Boston Scientific, and Medtronic. Dr. Weinsaft has received speaker honoraria from GE Healthcare. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
Assessment of Secondary Mitral Regurgitation: Is Cardiovascular Magnetic Resonance 1-Stop Shop Imaging Technique?JACC Cardiovasc Imaging. 2021 Apr;14(4):840-842. doi: 10.1016/j.jcmg.2021.01.021. Epub 2021 Mar 17. JACC Cardiovasc Imaging. 2021. PMID: 33744140 No abstract available.
References
-
- Groarke JD CB, O’Gara PT, Fuster V, Harrington RA, Narula J, Eapen ZJ. Ischemic Mitral Regurgitation. In: H JW, editor Hurst’s The Heart. 14 ed. New York, NY: McGraw-Hill Education, 2017.
-
- Grigioni F, Enriquez-Sarano M, Zehr KJ, Bailey KR, Tajik AJ. Ischemic mitral regurgitation: long-term outcome and prognostic implications with quantitative Doppler assessment. Circulation 2001;103:1759–64. - PubMed
-
- Bursi F, Enriquez-Sarano M, Nkomo VT et al. Heart failure and death after myocardial infarction in the community: the emerging role of mitral regurgitation. Circulation 2005;111:295–301. - PubMed
-
- Perez de Isla L, Zamorano J, Quezada M et al. Functional mitral regurgitation after a first non-ST-segment elevation acute coronary syndrome: contribution to congestive heart failure. Eur Heart J 2007;28:2866–72. - PubMed
-
- Cavalcante JL, Kusunose K, Obuchowski NA et al. Prognostic Impact of Ischemic Mitral Regurgitation Severity and Myocardial Infarct Quantification by Cardiovascular Magnetic Resonance. JACC Cardiovasc Imaging 2019. - PubMed
Publication types
MeSH terms
Grants and funding
- R01 HL141917/HL/NHLBI NIH HHS/United States
- K23 HL140092/HL/NHLBI NIH HHS/United States
- P30 CA008748/CA/NCI NIH HHS/United States
- R01 HL128278/HL/NHLBI NIH HHS/United States
- R01 HL063348/HL/NHLBI NIH HHS/United States
- T32 HL007854/HL/NHLBI NIH HHS/United States
- T32 HL160520/HL/NHLBI NIH HHS/United States
- R01 HL151686/HL/NHLBI NIH HHS/United States
- K23 HL132011/HL/NHLBI NIH HHS/United States
- R01 HL128099/HL/NHLBI NIH HHS/United States
- R61 HL151355/HL/NHLBI NIH HHS/United States
- K23 HL102249/HL/NHLBI NIH HHS/United States
- R33 HL151355/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
