

Impaired Coronary Vasodilator Reserve and Adverse Prognosis in Patients With Systemic Inflammatory Disorders
- PMID: 33744132
- PMCID: PMC8429517
- DOI: 10.1016/j.jcmg.2020.12.031
Impaired Coronary Vasodilator Reserve and Adverse Prognosis in Patients With Systemic Inflammatory Disorders
Abstract
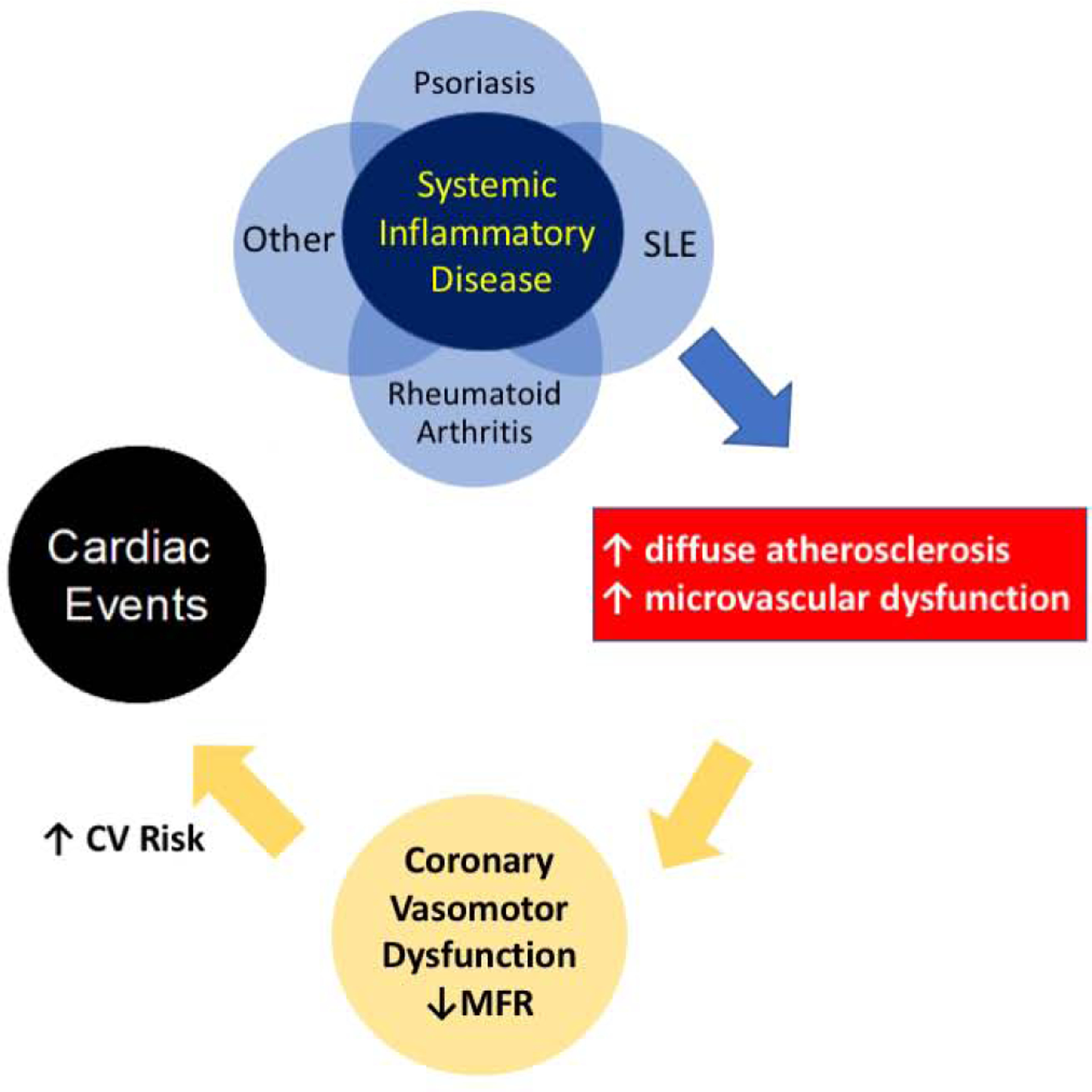
Objectives: The purpose of this study was to evaluate the prognostic value of quantitative myocardial blood flow (MBF) and myocardial flow reserve (MFR), reflecting the integrated effects of diffuse atherosclerosis and microvascular dysfunction in patients with systemic inflammatory disorders.
Background: Rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), and psoriasis (PsO) are common inflammatory conditions with excess cardiovascular (CV) risk compared to the general population. Systemic inflammation perturbs endothelial function and has been linked to coronary vasomotor dysfunction. However, the prognostic significance of this vascular dysfunction is not known.
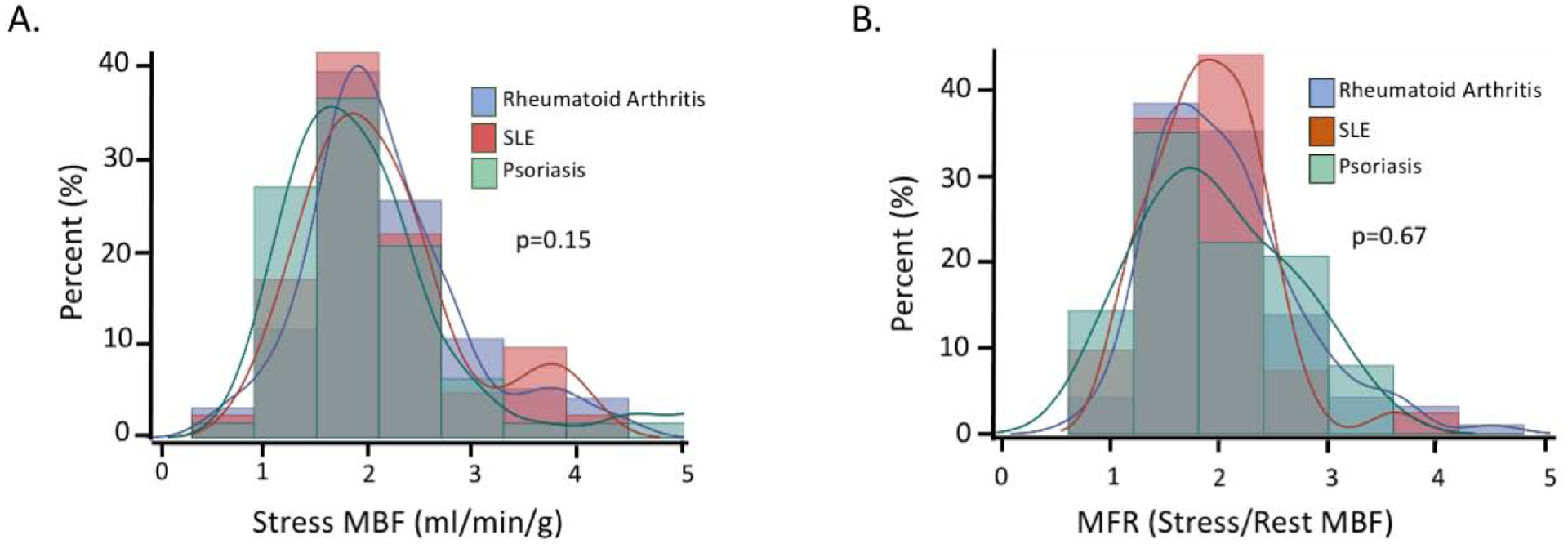
Methods: This was a retrospective study of patients with RA, SLE, and PsO undergoing clinically indicated rest and stress myocardial perfusion positron emission tomography (PET). Patients with an abnormal myocardial perfusion study or left ventricular dysfunction were excluded. MFR was calculated as the ratio of myocardial blood flow (MBF, ml/min/g) at peak stress compared to that at rest.
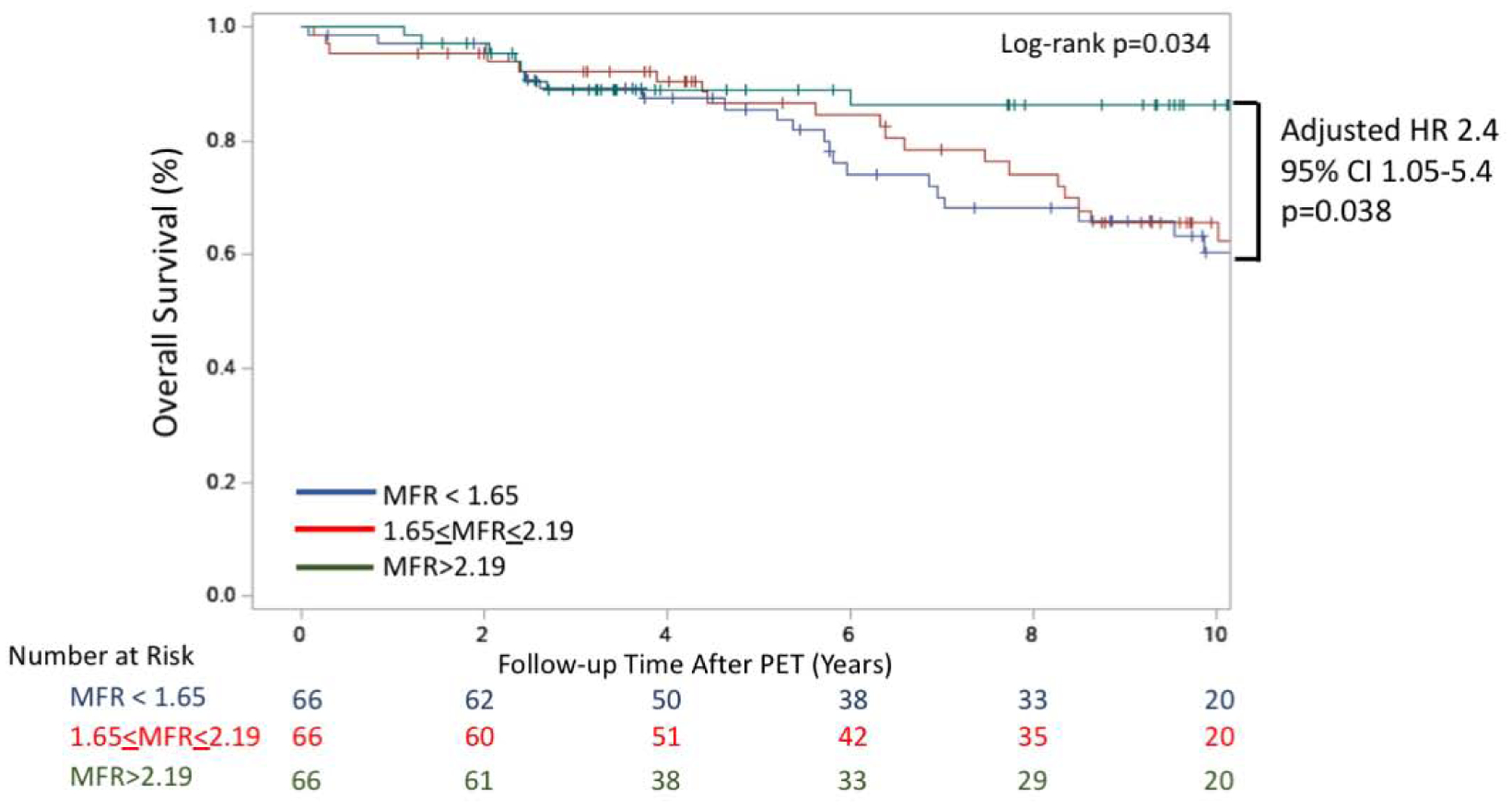
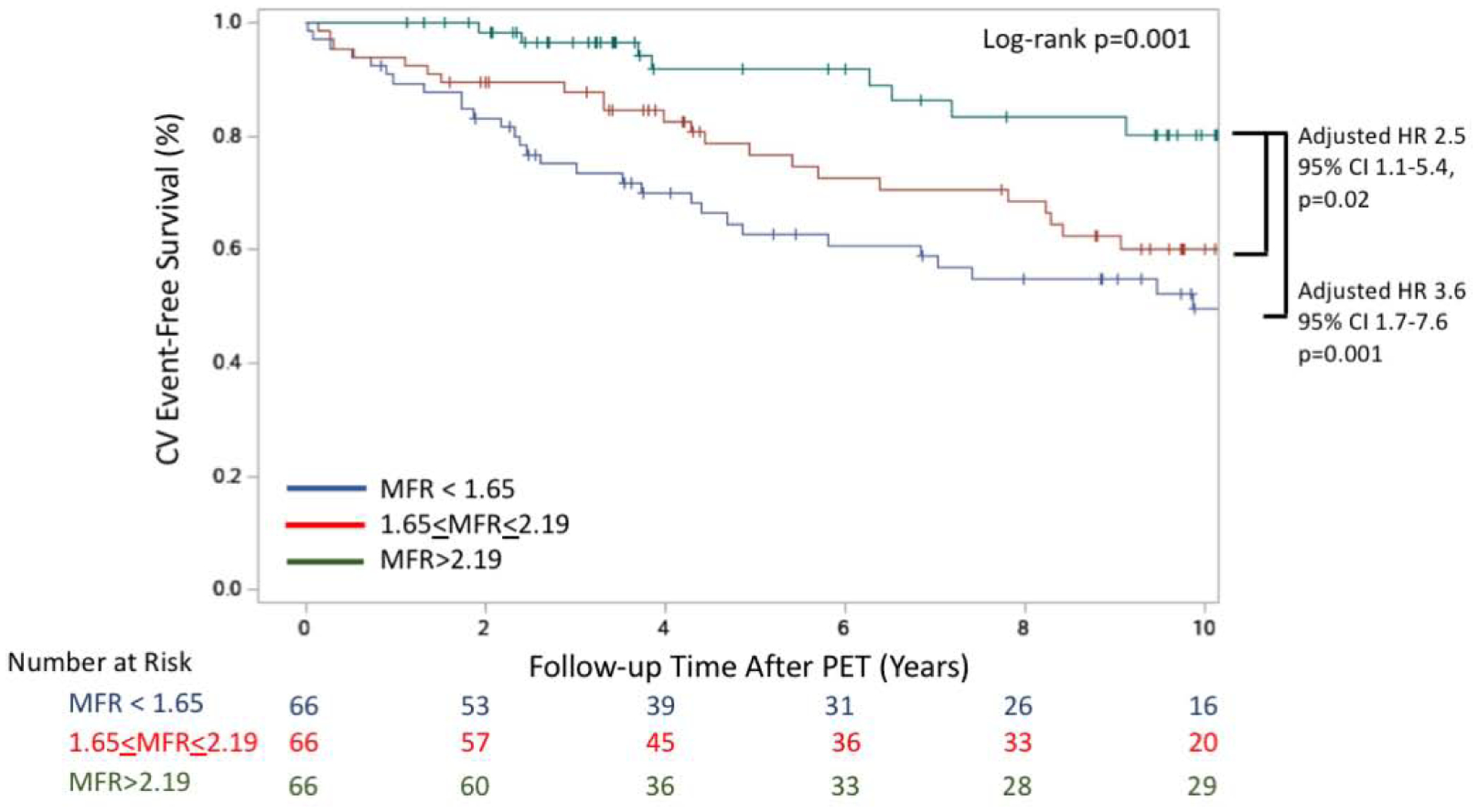
Results: Among the 198 patients (median age: 65 years; 80% female), 20.7% had SLE, 31.8% had PsO, and 47.5% had RA. There were no differences in mean MFR between these conditions. Over a median follow-up of 7.8 years, there were 51 deaths and 63 major adverse cardiovascular events (MACE). Patients in the lowest tertile (MFR <1.65) had higher all-cause mortality than the highest tertile, which remained significant after adjusting for age, sex, and the pre-test clinical risk score (hazard ratio [HR]: 2.4; 95% confidence interval [CI]: 1.05 to 5.4; p = 0.038). Similarly, compared to the highest MFR tertile, those in the lowest tertile had a lower MACE-free survival after adjusting for age, sex, and the pre-test clinical risk score (HR: 3.6; 95% CI: 1.7 to 7.6; p = 0.001).
Conclusions: In patients with systemic inflammatory disorders, impaired coronary vasodilator reserve was associated with worse cardiovascular outcomes and all-cause mortality.
Keywords: PET; inflammation; microvascular dysfunction; nuclear imaging.
Copyright © 2021 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures Supported by National Heart, Lung, and Blood Institute (NHLBI) grant T32 HL094301 (Drs Weber and Divakaran), grant T32 T32HL007604 (Dr Brown), National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS) grant K24 AR066109 (Dr Costenbader), National Institutes of Health (NIH) grant K23 HL135438 (Dr Taqueti), and National Heart, Lung, and Blood Institute grant R01HL150342 (Dr Divakaran). Dr Di Carli has received grants from Gilead Sciences and Spectrum Dynamics; and is a consultant for Janssen and Bayer, outside the submitted work. Dr Dorbala has received grants from Pfizer and GE Healthcare; and is a consultant for GE Healthcare and Pfizer, outside the submitted work. Dr Blankstein has received grants from Amgen and Astellas; and is a consultant for Amgen, outside of the submitted work. Dr Merola has received grants from and is a consultant for Merck, Abbvie, Dermavant, Eli Lilly, Novartis, Janssen, Union Chimique Belge (UCB), Celgene, Sanofi, Regeneron, Arena, Sun Pharma, Biogen, Pfizer, EMD Sorono, Avotres, and Leo Pharma. Dr Massarotti has received grants from Bristol-Myers Squibb; and is a consultant for UCB and Exagen; and serves on data safety monitoring board for EMD Serono. Dr Costenbader has received grants from Merck, AstraZeneca, Janssen, and Glaxo Smith Kline; and is a consultant for Merck. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
Epicardial Assessment of Coronary Artery Disease in Inflammatory Diseases: Is it Enough?JACC Cardiovasc Imaging. 2021 Nov;14(11):2221-2225. doi: 10.1016/j.jcmg.2021.02.013. Epub 2021 Apr 14. JACC Cardiovasc Imaging. 2021. PMID: 33865786 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
