

A Refinement of Clinical Tumor Marker Monitoring: Why Not Use an Inverse Value of Doubling Time?
- PMID: 33744875
- PMCID: PMC8280408
- DOI: 10.1159/000515977
A Refinement of Clinical Tumor Marker Monitoring: Why Not Use an Inverse Value of Doubling Time?
Abstract
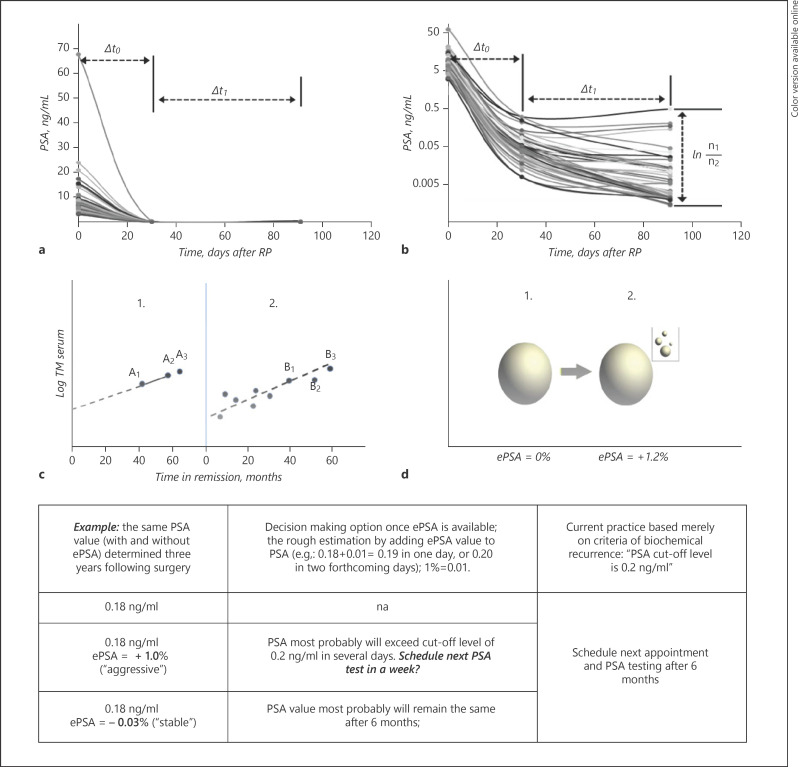
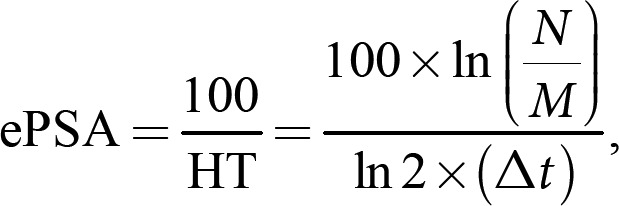
Objectives: The aim of this study was to compare prostate-specific antigen (PSA) kinetics - half-life time (HT), doubling time (DT), and elimination rate PSA (ePSA) in prostate cancer (PCa) monitoring. Implementation of ePSA in clinical practice could help simplify patient monitoring in the remission phase.
Materials and methods: A total of 49 PCa patients were examined by their PSA tests before prostatectomy and after 30 days, 91 days, and 24 months. Conventional PSA rate of change parameters (HT and DT) were compared to a new clinically understandable ePSA parameter.
Results: We observed that implementation of inverse value (ePSA) rather than HT or DT has distinct advantages: (1) values are valid when PSA is unchanged (ePSA equals zero), (2) the concept of ePSA can be easily understood, as it is a growth fraction, (3) ePSA fluctuates within a narrow range and is thus easy to interpret, and (4) there are no mathematical flaws (no positive skewing).
Conclusion: Exploring ePSA norm as ≤0% could help spot biochemical recurrence in a timely manner. Primary health care providers tend to use an irrelevant PSA threshold, that is, 4.0 ng/mL, in postoperative follow-up. The delayed referrals of patients in remission might be reduced if ePSA testing is adopted.
Keywords: Cancer relapse; Prostate cancer; Prostate-specific antigen; Tumor markers.
© 2021 The Author(s). Published by S. Karger AG, Basel.
Conflict of interest statement
The authors have nothing to declare.
Figures
References
-
- Wilder JL, Pavlik E, Straughn JM, Kirby T, Higgins RV, DePriest PD, et al. Clinical implications of a rising serum CA-125 within the normal range in patients with epithelial ovarian cancer: a preliminary investigation. Gynecol Oncol. 2003 May;89((2)):233–5. - PubMed
-
- Freedland SJ, Humphreys EB, Mangold LA, Eisenberger M, Dorey FJ, Walsh PC, et al. Risk of prostate cancer-specific mortality following biochemical recurrence after radical prostatectomy. JAMA. 2005 Jul 27;294((4)):433–9. - PubMed
-
- Mehrara E, Forssell-Aronsson E, Ahlman H, Bernhardt P. Specific growth rate versus doubling time for quantitative characterization of tumor growth rate. Cancer Res. 2007 Apr 15;67((8)):3970–5. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
