

Transvenous phrenic nerve stimulation improves central sleep apnea, sleep quality, and quality of life regardless of prior positive airway pressure treatment
- PMID: 33745107
- PMCID: PMC8590675
- DOI: 10.1007/s11325-021-02335-x
Transvenous phrenic nerve stimulation improves central sleep apnea, sleep quality, and quality of life regardless of prior positive airway pressure treatment
Abstract
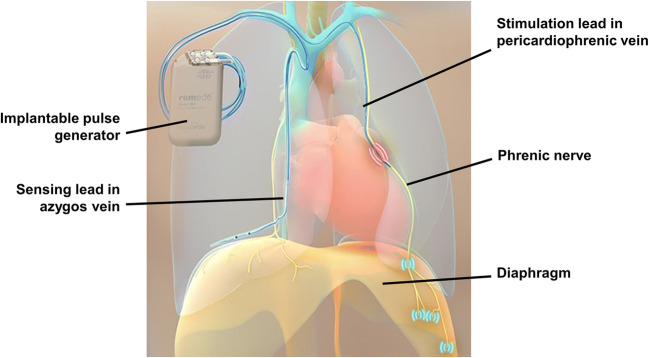
Study objective: Positive airway pressure (PAP) therapy for central sleep apnea (CSA) is often poorly tolerated, ineffective, or contraindicated. Transvenous phrenic nerve stimulation (TPNS) offers an alternative, although its impact on previously PAP-treated patients with CSA has not been examined.
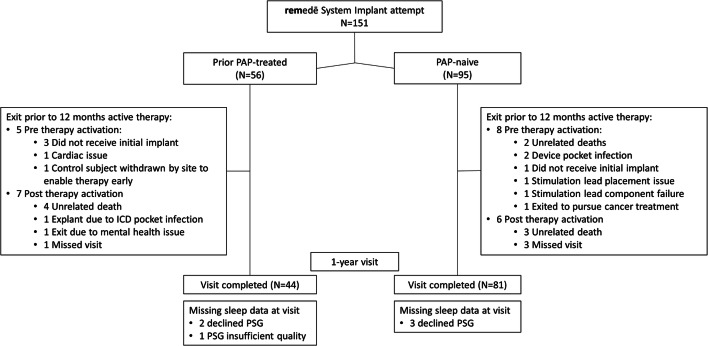
Methods: TPNS responses among PAP-naïve and prior PAP-treated patients from the remedē® System Pivotal Trial were assessed. Of 151, 56 (37%) used PAP therapy before enrolling in the trial. Patients were implanted with a TPNS device and randomized to either active or deferred (control) therapy for 6 months before therapy activation. Apnea-hypopnea index (AHI) and patient-reported outcomes (PRO) were assessed at baseline, and 6 and 12 months following active therapy.
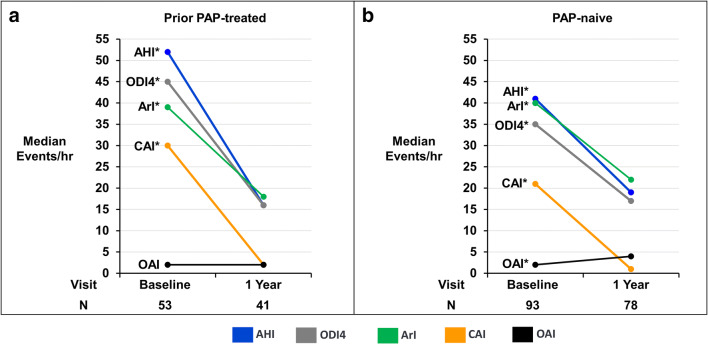
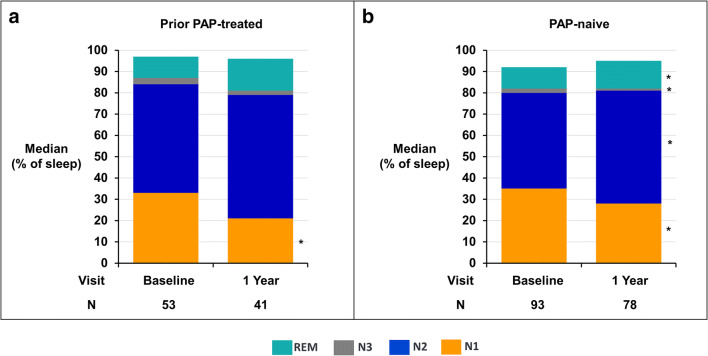
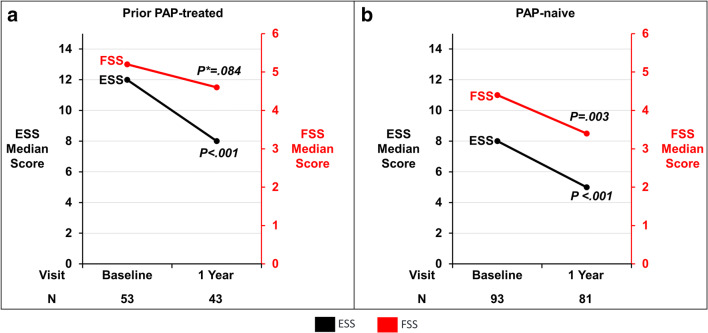
Results: Patients had moderate-severe CSA at baseline, which was of greater severity and more symptomatic in the PAP-treated vs. PAP-naïve group (median AHI 52/h vs. 38, central apnea index (CAI) 32/h vs. 18, Epworth Sleepiness Scale 13 vs. 10, fatigue severity scale 5.2 vs. 4.5). Twelve months of TPNS decreased AHI to <20/h and CAI to ≤2/h. Both groups showed reductions in daytime sleepiness and fatigue, improved well-being by patient global assessment, and high therapeutic acceptance with 98% and 94% of PAP-treated and PAP-naïve patients indicating they would undergo the implant again. Stimulation produced discomfort in approximately one-third of patients, yet <5% of prior PAP-treated participants discontinued therapy.
Conclusion: Polysomnographic and clinical responses to TPNS were comparable in PAP-naïve and prior PAP-treated CSA patients. TPNS is a viable therapy across a broad spectrum of CSA patients.
Trial registration: ClinicalTrials.gov Identifier NCT01816776; March 22, 2013.
Keywords: Central sleep apnea; Positive airway pressure; Transvenous phrenic nerve stimulation.
© 2021. The Author(s).
Conflict of interest statement
The authors have the following conflicts of interest to declare: Schwartz: consulting fees from Respicardia. Goldberg: received research grants and consulting fees from Respicardia. McKane: employee of Respicardia where he is a statistician. Morgenthaler: consulting fees from Respicardia.
Figures
References
-
- Marin JM, Carrizo SJ, Vicente E, Agusti AG. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet. 2005;365(9464):1046–1053. doi: 10.1016/S0140-6736(05)71141-7. - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
