

Myeloablative Haploidentical Transplant as an Alternative to Matched Sibling Transplant for Peripheral T-Cell Lymphomas
- PMID: 33745341
- PMCID: PMC7989122
- DOI: 10.1177/0963689721999615
Myeloablative Haploidentical Transplant as an Alternative to Matched Sibling Transplant for Peripheral T-Cell Lymphomas
Abstract
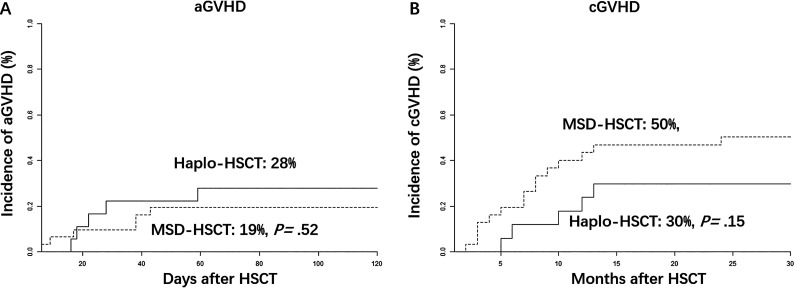
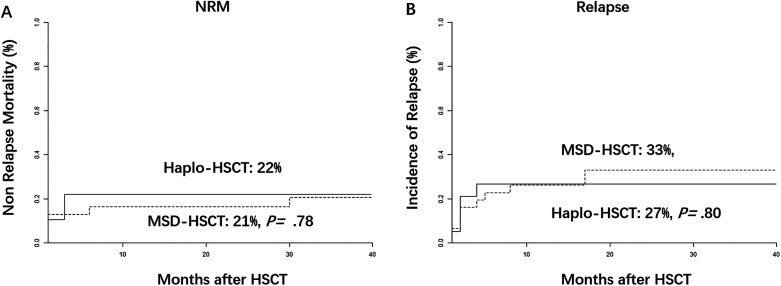
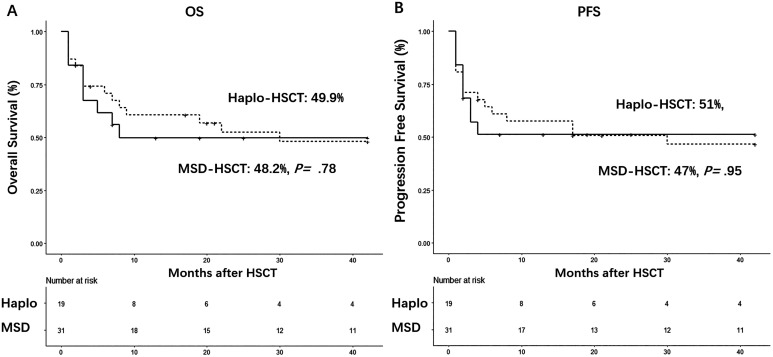
The number of HLA-haploidentical allogeneic hematopoietic stem-cell transplantation (Haplo-HSCT) is increasing. Comparative studies about Haplo-HSCT versus allo-HSCT with HLA-matched sibling donors (MSD-HSCT) have been tried in leukemias and B-cell lymphomas. Few studies were reported in Peripheral T-cell lymphomas (PTCLs). We performed a multicenter retrospective study about 52 patients with PTCLs undergoing Haplo-HSCT (n = 20) or MSD-HSCT (n = 32). All Haplo-HSCT recipients received antithymocyte globulin (ATG) based graft versus host disease (GVHD) prophylaxis. The median follow-up for all survivors was 38 months. The 100-day cumulative incidence of grade II to IV acute GVHD was similar (19% in the MSD-HSCT group versus 28% in the Haplo-HSCT group, P = 0.52). The 2-year cumulative incidence of chronic GVHD (limited and extensive) after Haplo-HSCT (30%) was also similar with that in the MSD-HSCT group (50%, P = 0.15). The 3-year relapse rates (33% vs 27%, P = 0.84) and non-relapse mortality (21% vs 22%, P = 0.78) did not differ between these two groups. There were also no differences in 3-year overall survival (OS) (48% vs 50%, P = 0.78) and progression-free survival (47% vs 51%, P = 0.95) between these two groups. On multivariate analysis, prognostic index for T-cell lymphoma (PIT) score (higher than 1: hazard ratio [HR], 4.0; P = 0.003) and disease status (stable or progression disease before HSCT: HR, 2.8; P = 0.03) were independent variables associated with worse OS. We concluded that ATG-based haplo-HSCT platform could work as an alternative to MSD-HSCT for patients with PTCLs.
Keywords: HLA-matched sibling donor; allo-HSCT; antithymocyte globulin; haploidentical donor; peripheral t-cell lymphoma.
Conflict of interest statement
Figures
References
-
- Vose J, Armitage J, Weisenburger D; International T-Cell Lymphoma Project. International peripheral T-cell and natural killer/T-cell lymphoma study: pathology findings and clinical outcomes. J Clin Oncol. 2008;26(25):4124–4130. - PubMed
-
- Kwong YL, Anderson BO, Advani R, Kim WS, Levine AM, Lim ST; Asian Oncology Summit. Management of T-cell and natural-killer-cell neoplasms in Asia: consensus statement from the Asian Oncology Summit 2009. Lancet Oncol. 2009;10(11):1093–1101. - PubMed
-
- Tse E, Kwong YL. How I treat NK/T-cell lymphomas. Blood. 2013;121(25):4997–5005. - PubMed
-
- Ellin F, Landstrom J, Jerkeman M, Relander T. Real-world data on prognostic factors and treatment in peripheral T-cell lymphomas: a study from the Swedish Lymphoma Registry. Blood. 2014;124(10):1570–1577. - PubMed
-
- Mak V, Hamm J, Chhanabhai M, Shenkier T, Klasa R, Sehn LH, Villa D, Gascoyne RD, Connors JM, Savage KJ. Survival of patients with peripheral T-cell lymphoma after first relapse or progression: spectrum of disease and rare long-term survivors. J Clin Oncol. 2013;31(16):1970–1976. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
