

Left atrial 4D flow cardiovascular magnetic resonance: a reproducibility study in sinus rhythm and atrial fibrillation
- PMID: 33745457
- PMCID: PMC7983287
- DOI: 10.1186/s12968-021-00729-0
Left atrial 4D flow cardiovascular magnetic resonance: a reproducibility study in sinus rhythm and atrial fibrillation
Abstract
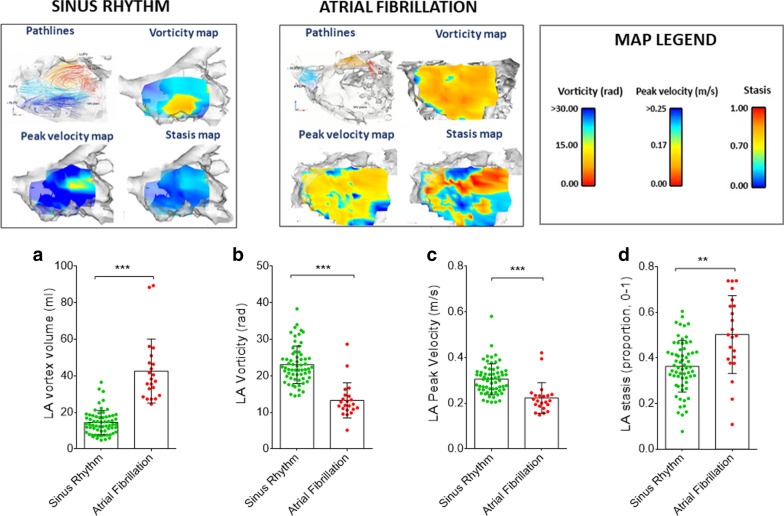
Background: Four-dimensional (4D) flow cardiovascular magnetic resonance (CMR) allows sophisticated quantification of left atrial (LA) blood flow, and could yield novel biomarkers of propensity for intra-cardiac thrombus formation and embolic stroke. As reproducibility is critically important to diagnostic performance, we systematically investigated technical and temporal variation of LA 4D flow in atrial fibrillation (AF) and sinus rhythm (SR).
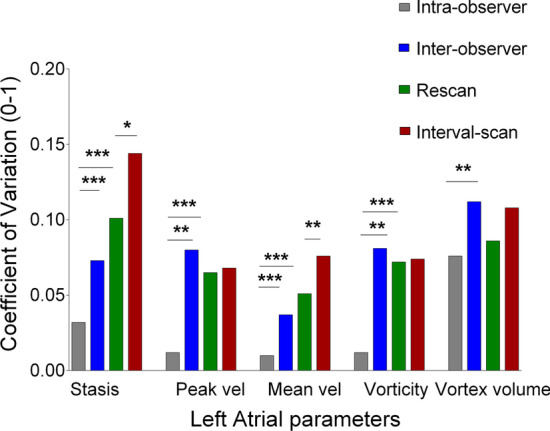
Methods: Eighty-six subjects (SR, n = 64; AF, n = 22) with wide-ranging stroke risk (CHA2DS2VASc 0-6) underwent LA 4D flow assessment of peak and mean velocity, vorticity, vortex volume, and stasis. Eighty-five (99%) underwent a second acquisition within the same session, and 74 (86%) also returned at 30 (27-35) days for an interval scan. We assessed variability attributable to manual contouring (intra- and inter-observer), and subject repositioning and reacquisition of data, both within the same session (same-day scan-rescan), and over time (interval scan). Within-subject coefficients of variation (CV) and bootstrapped 95% CIs were calculated and compared.
Results: Same-day scan-rescan CVs were 6% for peak velocity, 5% for mean velocity, 7% for vorticity, 9% for vortex volume, and 10% for stasis, and were similar between SR and AF subjects (all p > 0.05). Interval-scan variability was similar to same-day scan-rescan variability for peak velocity, vorticity, and vortex volume (all p > 0.05), and higher for stasis and mean velocity (interval scan CVs of 14% and 8%, respectively, both p < 0.05). Longitudinal changes in heart rate and blood pressure at the interval scan in the same subjects were associated with significantly higher variability for LA stasis (p = 0.024), but not for the remaining flow parameters (all p > 0.05). SR subjects showed significantly greater interval-scan variability than AF patients for mean velocity, vortex volume, and stasis (all p < 0.05), but not peak velocity or vorticity (both p > 0.05).
Conclusions: LA peak velocity and vorticity are the most reproducible and temporally stable novel LA 4D flow biomarkers, and are robust to changes in heart rate, blood pressure, and differences in heart rhythm.
Keywords: 4D flow; Cardioembolic risk; Cardiovascular magnetic resonance; Left atrium; Reproducibility; Stasis; Velocities; Vortex; Vorticity.
Conflict of interest statement
BC is receiving support in kind from Roche Diagnostics (blood assays) and iRhythm (ECG monitors) in clinical studies on atrial fibrillation. RW has received honoraria and/or travel assistance from Biosense Webster, Bayer, Boston Scientific and Abbott. All authors report no conflicts of interest in relation to this work.
Figures
References
-
- Handke M, Harloff A, Hetzel A, Olschewski M, Bode C, Geibel A. Left atrial appendage flow velocity as a quantitative surrogate parameter for thromboembolic risk: determinants and relationship to spontaneous echocontrast and thrombus formation—a transesophageal echocardiographic study in 500 patients with cerebral ischemia. J Am Soc Echocardiogr. 2005;18:1366–72. doi: 10.1016/j.echo.2005.05.006. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
