

Evaluation of artificial intelligence systems for assisting neurologists with fast and accurate annotations of scalp electroencephalography data
- PMID: 33745882
- PMCID: PMC8105505
- DOI: 10.1016/j.ebiom.2021.103275
Evaluation of artificial intelligence systems for assisting neurologists with fast and accurate annotations of scalp electroencephalography data
Abstract
Background: Assistive automatic seizure detection can empower human annotators to shorten patient monitoring data review times. We present a proof-of-concept for a seizure detection system that is sensitive, automated, patient-specific, and tunable to maximise sensitivity while minimizing human annotation times. The system uses custom data preparation methods, deep learning analytics and electroencephalography (EEG) data.
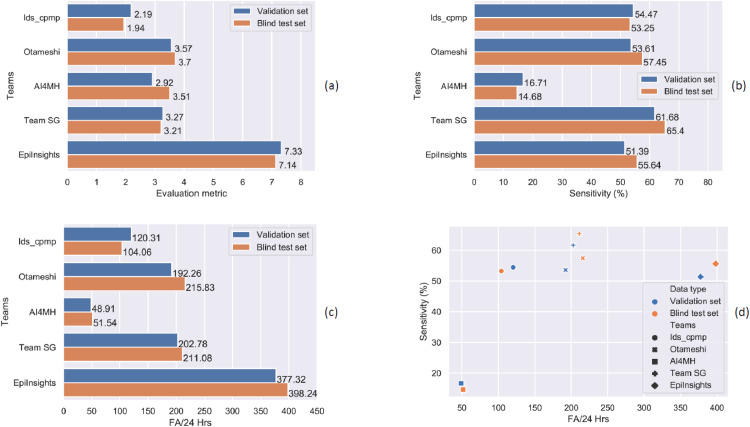
Methods: Scalp EEG data of 365 patients containing 171,745 s ictal and 2,185,864 s interictal samples obtained from clinical monitoring systems were analysed as part of a crowdsourced artificial intelligence (AI) challenge. Participants were tasked to develop an ictal/interictal classifier with high sensitivity and low false alarm rates. We built a challenge platform that prevented participants from downloading or directly accessing the data while allowing crowdsourced model development.
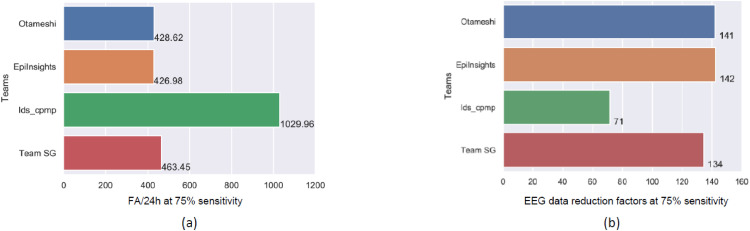
Findings: The automatic detection system achieved tunable sensitivities between 75.00% and 91.60% allowing a reduction in the amount of raw EEG data to be reviewed by a human annotator by factors between 142x, and 22x respectively. The algorithm enables instantaneous reviewer-managed optimization of the balance between sensitivity and the amount of raw EEG data to be reviewed.
Interpretation: This study demonstrates the utility of deep learning for patient-specific seizure detection in EEG data. Furthermore, deep learning in combination with a human reviewer can provide the basis for an assistive data labelling system lowering the time of manual review while maintaining human expert annotation performance.
Funding: IBM employed all IBM Research authors. Temple University employed all Temple University authors. The Icahn School of Medicine at Mount Sinai employed Eren Ahsen. The corresponding authors Stefan Harrer and Gustavo Stolovitzky declare that they had full access to all the data in the study and that they had final responsibility for the decision to submit for publication.
Keywords: Artificial intelligence; Automatic labelling, Crowdsourcing challenges; Deep neural networks; EEG; Epilepsy; Seizure detection.
Copyright © 2021 The Authors. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest SR, IKK and SH are inventors on issued patent US 10,596,377. HY is an inventor on pending patent US 16/670,177. All other authors do report no conflicts of interest.
Figures





Comment in
-
Bring the model to the data: The Deep Learning Epilepsy Detection Challenge.EBioMedicine. 2021 Apr;66:103323. doi: 10.1016/j.ebiom.2021.103323. Epub 2021 Apr 12. EBioMedicine. 2021. PMID: 33857902 Free PMC article. No abstract available.
References
-
- Gulshan V., Peng L., Coram M. Development and validation of a deep learning algorithm for detection of diabetic retinopathy in retinal fundus photographs. JAMA. 2016;316(22):2402–2410. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
