

A Systematic Review of Monogenic Inflammatory Bowel Disease
- PMID: 33746097
- PMCID: PMC8448782
- DOI: 10.1016/j.cgh.2021.03.021
A Systematic Review of Monogenic Inflammatory Bowel Disease
Abstract
Background & aims: Advances in genomic technologies have led to increasing reports of monogenic inflammatory bowel disease (IBD). Here, we systematically review the literature to determine the clinical features, genetic profile, and previously used treatment strategies in monogenic IBD.
Methods: A systematic review of MEDLINE articles published between January 2000 and December 2020 was conducted. A total of 750 individual monogenic IBD cases were identified from 303 eligible articles.
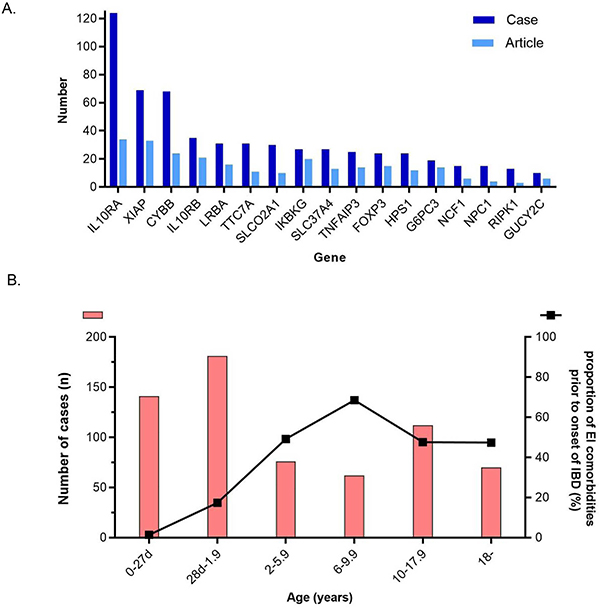
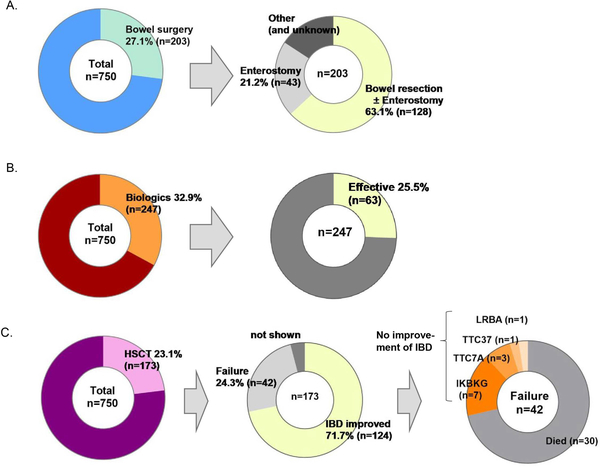
Results: The most frequently reported monogenic IBD genes were IL10RA/B, XIAP, CYBB, LRBA, and TTC7A. In total, 63.4% of patients developed IBD before 6 years of age, 17.4% developed IBD between ages 10 and 17.9 years, and 10.9% developed IBD after age 18. There was a substantial difference between these age groups and the underlying monogenic disorders. Only 31.7% had any history of extraintestinal comorbidity (EIC) before IBD onset, but 76.0% developed at least 1 EIC during their clinical course. The most common EICs were atypical infection (44.7%), dermatologic abnormality (38.4%), and autoimmunity (21.9%). Bowel surgery, biologic therapy, and hematopoietic stem cell transplantation were performed in 27.1%, 32.9%, and 23.1% of patients, respectively.
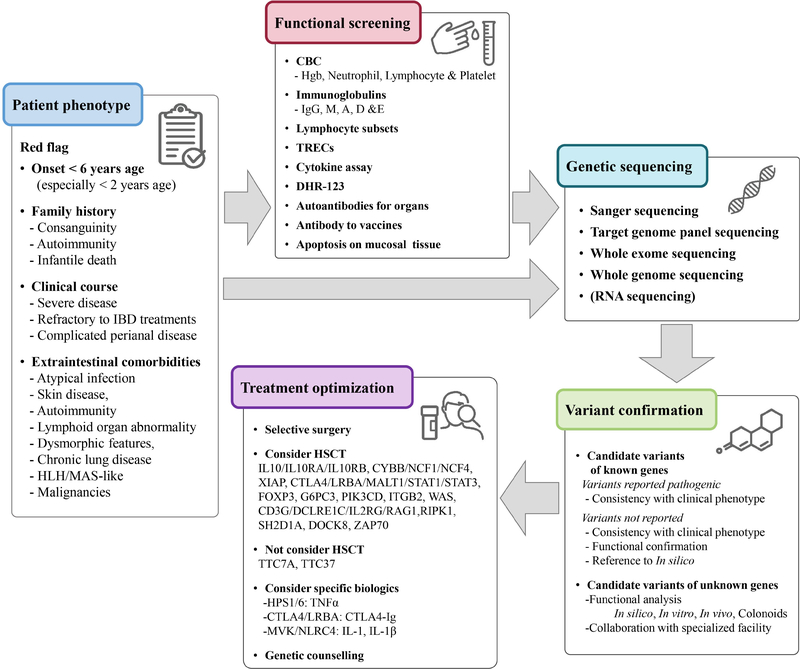
Conclusions: Monogenic IBD cases, although rare, have varied extraintestinal comorbidities and limited treatment options including surgery and transplant. Early identification and improved understanding of the characteristics of the genes and underlying disease processes in monogenic IBD is important for effective management.
Keywords: IBD; Monogenic Disorder; Pediatric; VEOIBD; Whole-Exome Sequence.
Copyright © 2022 The Authors. Published by Elsevier Inc. All rights reserved.
Figures


References
-
- Levine A, Koletzko S, Turner D, et al. ESPGHAN revised porto criteria for the diagnosis of inflammatory bowel disease in children and adolescents. J Pediatr Gastroenterol Nutr. 2014;58:795–806. - PubMed
-
- Sartor RB. Mechanisms of disease: pathogenesis of Crohn’s disease and ulcerative colitis. Nat Clin Pract Gastroenterol Hepatol 2006;3:390–407. - PubMed
-
- Muise AM, Snapper SB, Kugathasan S. The age of gene discovery in very early onset inflammatory bowel disease. Gastroenterology 2012;143:285–8. - PubMed
-
- Uhlig HH, Muise AM. Clinical Genomics in Inflammatory Bowel Disease. Trends Genet. 2017;33:629–641. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
