

Teriflunomide treatment is associated with optic nerve recovery in early multiple sclerosis
- PMID: 33747129
- PMCID: PMC7940774
- DOI: 10.1177/1756286421997372
Teriflunomide treatment is associated with optic nerve recovery in early multiple sclerosis
Abstract
Background and aims: Various attempts have been made to support recovery following optic neuritis (ON), but the respective trials have mostly been negative. The aim of this study was to determine whether disease-modifying treatment (DMT) following ON as first manifestation of relapsing-remitting multiple sclerosis influences long-term outcomes.
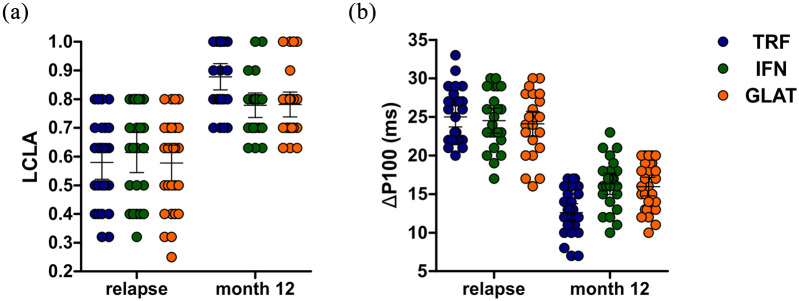
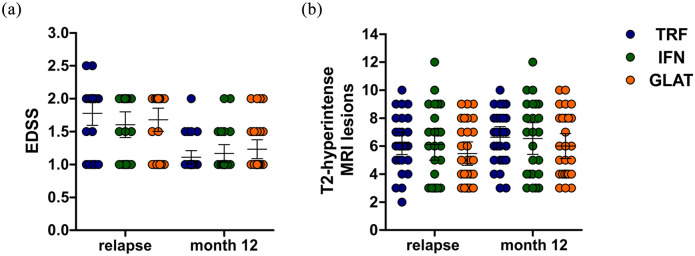
Methods: A total of 79 patients with ON were identified and evaluated at relapse, DMT induction, and 12 months following treatment induction with either glatiramer acetate (GLAT), interferon-beta (IFN), or teriflunomide (TRF). Low-contrast letter acuity (LCLA) and full-field visual-evoked potentials (FF-VEP) were compared between treatment groups using multivariable regression models. The impact of TRF treatment induction compared with IFN or GLAT following relapses outside the optic nerves was evaluated in an independent cohort of 122 patients. Magnetic resonance imaging (MRI) outcomes and rates of confirmed improvement of relapse-related disability were evaluated.
Results: TRF-treated patients exhibited higher LCLA and lower relative P100 latencies normalized to the fellow-eye. Findings were significant following covariate-adjustment by multivariable analyses. Cranial MRI lesion load as well as disability progression rates were not significantly different between groups. The cohort of patients following relapses other than ON showed no differences in confirmed improvement of disability.
Conclusion: TRF treatment is associated with favorable outcomes regarding functional optic nerve recovery following ON in early multiple sclerosis.
Keywords: disease-modifying treatment; multiple sclerosis; optic neuritis; teriflunomide.
© The Author(s), 2021.
Conflict of interest statement
Conflict of interest statement: Steffen Pfeuffer: received travel grants from Sanofi Genzyme and Merck Serono, lecturing honoraria from Sanofi Genzyme, Mylan Healthcare, and Biogen, and research support from Diamed, Merck Serono, and the German Multiple Sclerosis Society Northrhine-Westphalia. Laura Kerschke: declares no conflicts of interest Tobias Ruck: received travel grants and financial research support from Genzyme and Novartis and received honoraria for lecturing from Roche, Merck, Genzyme, Biogen, and Teva. Leoni Rolfes: received travel grants from Merck Serono and Sanofi-Genzyme. Marc Pawlitzki: received speaker honoraria and travel reimbursements from Novartis. Philipp Albrecht: received compensation for serving on Scientific Advisory Boards for Allergan, Biogen, Celgene, Ipsen, Merck Serono, Merz Pharmaceuticals, Novartis, and Roche. He received speaker honoraria and travel support from Allergan, Bayer Vital GmbH, Biogen, Celgene, Ipsen, Merck Serono, Merz Pharmaceuticals, Novartis, Roche. Philipp Albrecht received research support from Allergan, Biogen, Celgene, Ipsen, Merck Serono, Merz Pharmaceuticals, Novartis, and Roche. Heinz Wiendl: received compensation for serving on Scientific Advisory Boards/Steering Committees for Bayer Healthcare, Biogen Idec, Sanofi Genzyme, Merck Serono, and Novartis. He received speaker honoraria and travel support from Bayer Vital GmbH, Bayer Schering AG, Biogen, CSL Behring, EMD Serono, Fresenius Medical Care, Genzyme, Merck Serono, Omniamed, Novartis, and Sanofi Aventis. He received compensation as a consultant from Biogen Idec, Merck Serono, Novartis, Roche, and Sanofi-Genzyme. Heinz Wiendl also received research support from Bayer Healthcare, Bayer Vital, Biogen Idec, Merck Serono, Novartis, Sanofi Genzyme, Sanofi US, and Teva. Sven G. Meuth: received honoraria for lecturing and travel expenses for attending meetings from Almirall, Amicus Therapeutics Germany, Bayer Health Care, Biogen, Celgene, Diamed, Genzyme, MedDay Pharmaceuticals, Merck Serono, Novartis, Novo Nordisk, ONO Pharma, Roche, Sanofi-Aventis, Chugai Pharma, QuintilesIMS, and Teva. His research is funded by the German Ministry for Education and Research (BMBF), Deutsche Forschungsgemeinschaft (DFG), Else Kröner Fresenius Foundation, German Academic Exchange Service, Hertie Foundation, Interdisciplinary Center for Clinical Studies (IZKF) Muenster, German Foundation Neurology and by Almirall, Amicus Therapeutics Germany, Biogen, Diamed, Fresenius Medical Care, Genzyme, Merck Serono, Novartis, ONO Pharma, Roche, and Teva. The current work was conducted outside of third-party funding.
Figures
References
-
- Optic Neuritis Study Group. Visual function 15 years after optic neuritis: a final follow-up report from the optic neuritis treatment trial. Ophthalmology 2008; 115: 1079–1082.e5. - PubMed
-
- Cadavid D, Balcer L, Galetta S, et al. Safety and efficacy of opicinumab in acute optic neuritis (RENEW): a randomised, placebo-controlled, phase 2 trial. Lancet Neurol 2017; 16: 189–199. - PubMed
-
- Burman J, Raininko R, Fagius J. Bilateral and recurrent optic neuritis in multiple sclerosis. Acta Neurol Scand 2011; 123: 207–210. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
