

Impact of Pediatric Obesity on Diurnal Blood Pressure Assessment and Cardiovascular Risk Markers
- PMID: 33748038
- PMCID: PMC7969716
- DOI: 10.3389/fped.2021.596142
Impact of Pediatric Obesity on Diurnal Blood Pressure Assessment and Cardiovascular Risk Markers
Abstract
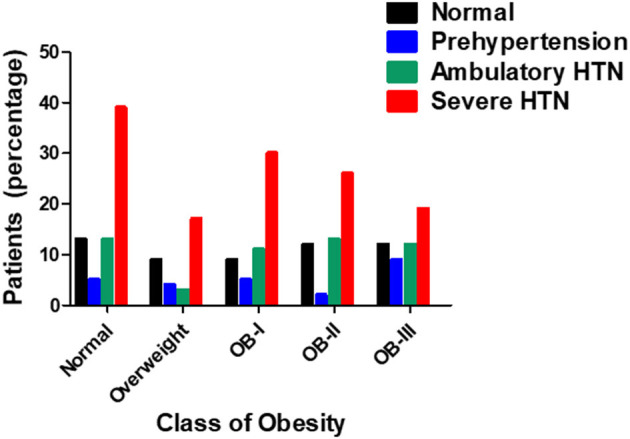
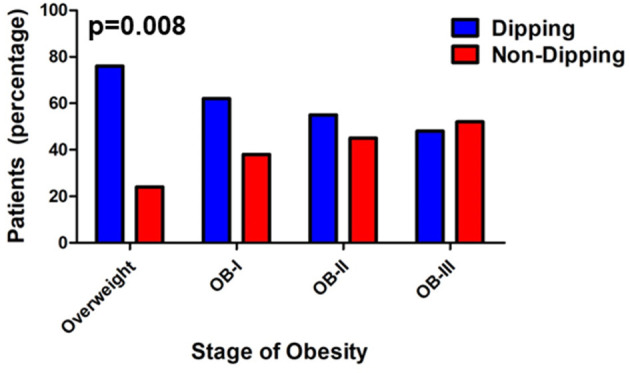
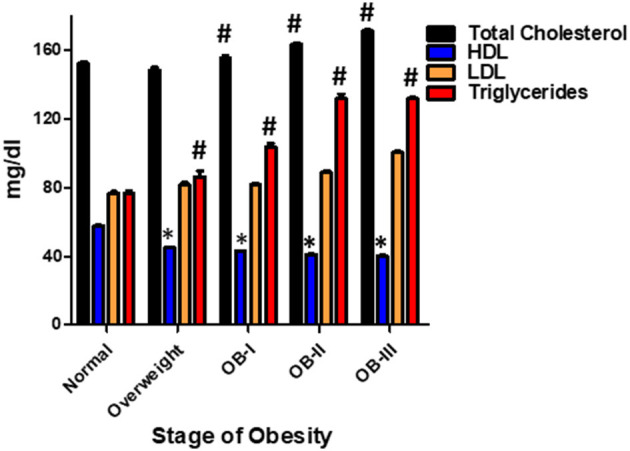
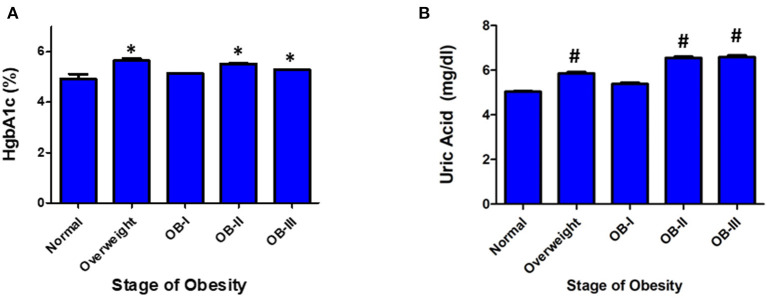
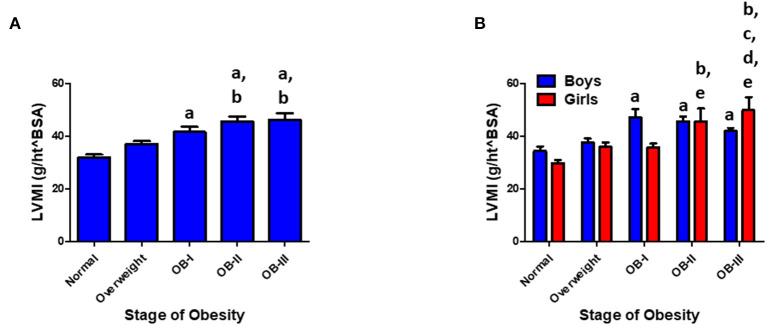
Background: The prevalence of hypertension is increasing particularly among obese children and adolescents. Obese children and adolescents with hypertension are likely to remain hypertensive as they reach adulthood and hypertension is linked to an increased risk for cardiovascular disease. Twenty-four-hour ambulatory blood pressure monitoring (ABPM) has become one of the most important tools in diagnosing hypertension in children and adolescents and circadian patterns of blood pressure may be important disease-risk predictors. Methods: A retrospective chart review was conducted in patients aged 6-21 years who underwent 24-h ABPM at Kentucky Children's Hospital (KCH) from August 2012 through June 2017. Exclusion criteria included conditions that could affect blood pressure including chronic kidney disease and other renal abnormalities, congenital heart disease, cancer, and thyroid disease. Subjects were categorized by body mass index into normal (below 85th percentile), overweight (85th-95th percentile), stage I obesity (95th-119th percentile), stage II obesity (120th-139th) and stage III obesity (>140th). Non-dipping was defined as a nocturnal BP reduction of <10%. Results: Two hundred and sixty-three patients (156 male patients) were included in the analysis, of whom 70 were normal weight, 33 overweight, 55 stage I obesity, 53 stage II, and 52 stage III obesity. Although there was no significant difference between normal weight and obese groups for prevalence of hypertension, there was a greater prevalence of SBP non-dipping in obese patients as BMI increased (p = 0.008). Furthermore, non-dippers had a significantly elevated LVMI as well as abnormal lab values for uric acid, blood lipid panel, creatinine, and TSH (p < 0.05). Conclusions: These findings demonstrate that obese children and adolescents constitute a large proportion of hypertensive children and adolescents and the severity of pediatric obesity is associated with nocturnal BP non-dipping. Additionally, obesity in children is linked to several cardiovascular risk factors including left ventricular hypertrophy, dyslipidemia, and elevated uric acid levels. Further studies utilizing ABPM measures on risk stratification in this very high-risk population are warranted.
Keywords: blood pressure; cardiovascular risk; left ventricular hypertrophy; nocturnal dipping; obesity; pediatric.
Copyright © 2021 Murphy, Huang, Bauer, Schadler, Makhoul, Clasey, Chishti and Kiessling.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Hales CM, Carroll MD, Fryar CD, Ogden CL. Prevalence of Obesity Among Adults and Youth: United States, 2015-2016. NCHS Data Brief. (2017). p. 1–8. Available online at: http://www.ncbi.nlm.nih.gov/pubmed/29155689 (accessed September 28, 2019). - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous