

Impact on the Gut Microbiota of Intensive and Prolonged Antimicrobial Therapy in Patients With Bone and Joint Infection
- PMID: 33748154
- PMCID: PMC7977441
- DOI: 10.3389/fmed.2021.586875
Impact on the Gut Microbiota of Intensive and Prolonged Antimicrobial Therapy in Patients With Bone and Joint Infection
Abstract
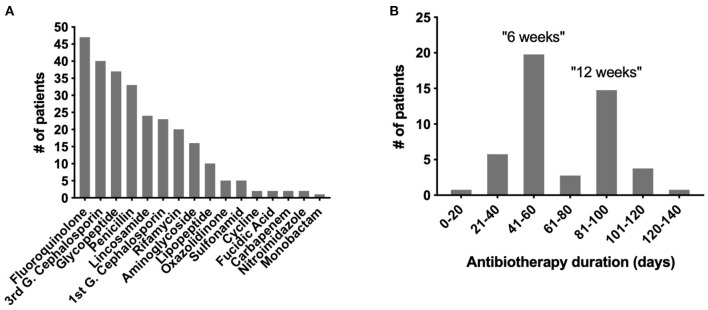
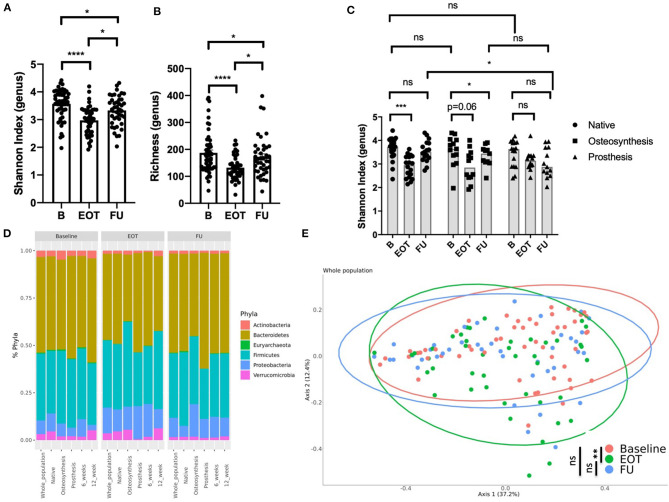
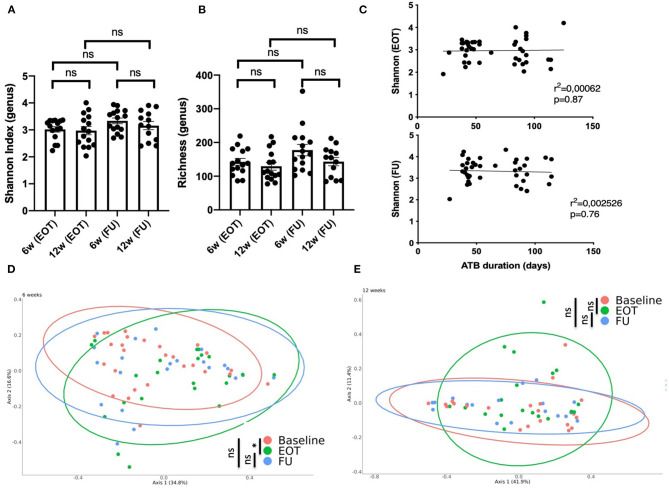
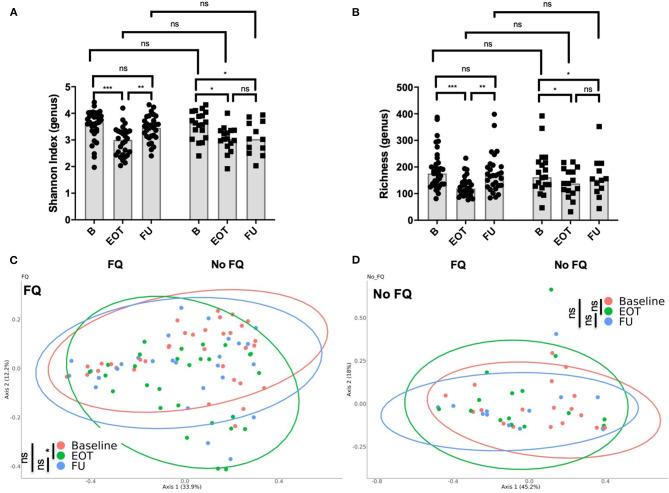
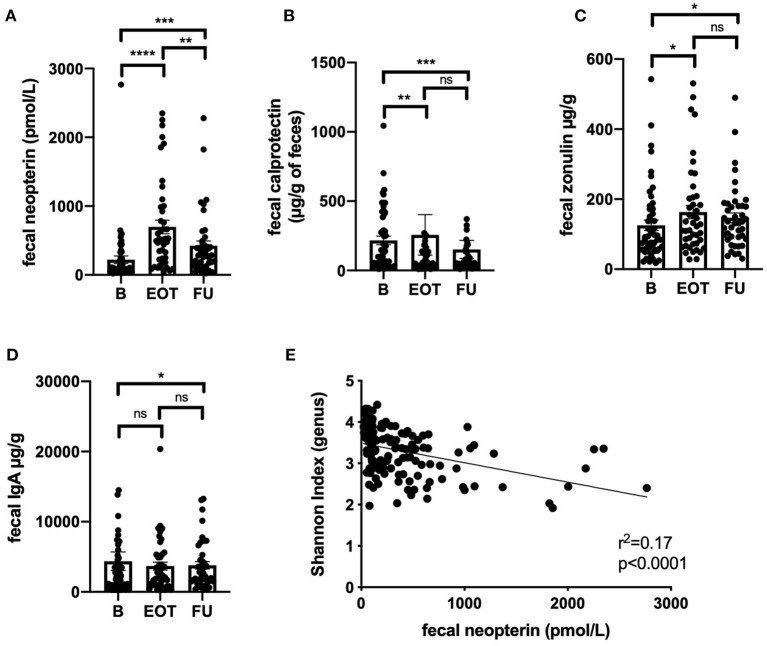
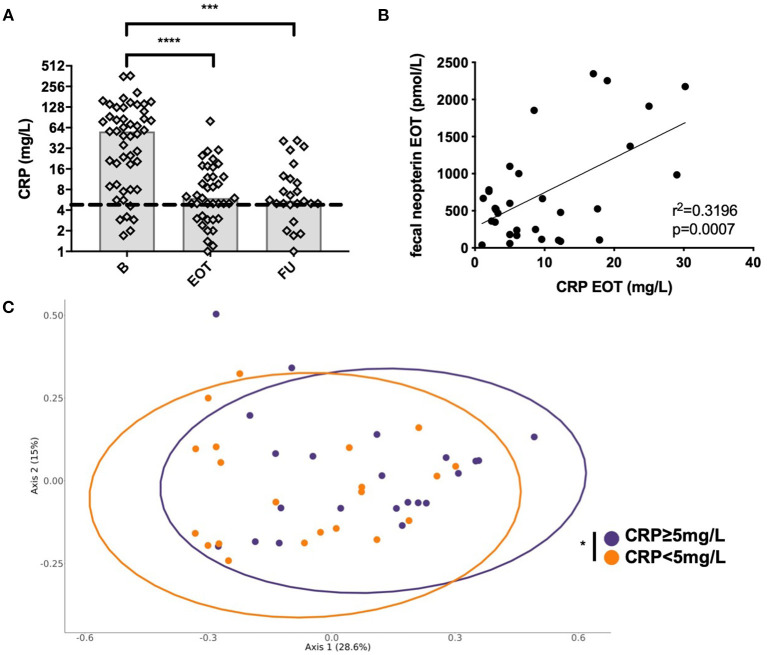
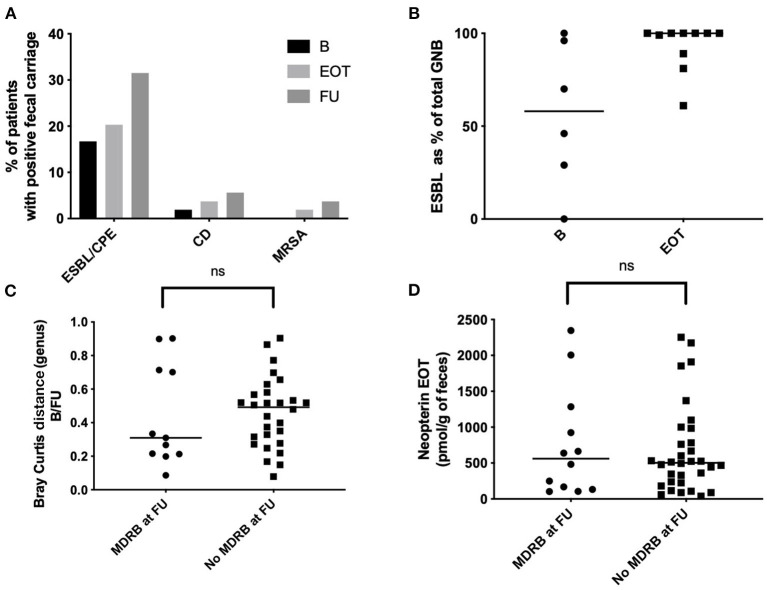
There is a growing interest in the potentially deleterious impact of antibiotics on gut microbiota. Patients with bone and joint infection (BJI) require prolonged treatment that may impact significantly the gut microbiota. We collected samples from patients with BJI at baseline, end of antibiotics (EOT), and 2 weeks after antibiotic withdrawal (follow-up, FU) in a multicenter prospective cohort in France. Microbiota composition was determined by shotgun metagenomic sequencing. Fecal markers of gut permeability and inflammation as well as multi-drug-resistant bacteria (MDRB) and Clostridioides difficile carriage were assessed at each time point. Sixty-two patients were enrolled: 27 native BJI, 14 osteosynthesis-related BJI, and 21 prosthetic joint infections (PJI). At EOT, there was a significant loss of alpha-diversity that recovered at FU in patients with native BJI and PJI, but not in patients with osteosynthesis-related BJI. At EOT, we observed an increase of Proteobacteria and Bacteroidetes that partially recovered at FU. The principal component analysis (PCoA) of the Bray-Curtis distance showed a significant change of the gut microbiota at the end of treatment compared to baseline that only partially recover at FU. Microbiota composition at FU does not differ significantly at the genus level when comparing patients treated for 6 weeks vs. those treated for 12 weeks. The use of fluoroquinolones was not associated with a lower Shannon index at the end of treatment; however, the PCoA of the Bray-Curtis distance showed a significant change at EOT, compared to baseline, that fully recovered at FU. Levels of fecal neopterin were negatively correlated with the Shannon index along with the follow-up (r 2 = 0.17; p < 0.0001). The PCoA analysis of the Bray-Curtis distance shows that patients with an elevated plasma level of C-reactive protein (≥5 mg/L) at EOT had a distinct gut microbial composition compared to others. MDRB and C. difficile acquisition at EOT and FU represented 20% (7/35) and 37.1% (13/35) of all MDRB/C. difficile-free patients at the beginning of the study, respectively. In patients with BJI, antibiotics altered the gut microbiota diversity and composition with only partial recovery, mucosal inflammation, and permeability and acquisition of MDRB carriage. Microbiome interventions should be explored in patients with BJI to address these issues.
Keywords: antibiotics; antimicrobial therapy; bone and joint infection; dysbiosis; gut microbiota.
Copyright © 2021 Levast, Benech, Gasc, Batailler, Senneville, Lustig, Pouderoux, Boutoille, Boucinha, Dauchy, Zeller, Maynard, Cazanave, Le Thi, Josse, Doré, Laurent and Ferry.
Conflict of interest statement
BL and CG are employed by the commercial company MaaT Pharma. LB was employed by the commercial company MaaT Pharma. NB declared a travel grant from Maat. JD is co-founder of MaaT Pharma. TF received advisory honorarium from MaaT Pharma and was the principal investigator of this study. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The authors declare that this study received funding from MaaT Pharma. The funder had the following involvement in the study: design, management and analysis.
Figures
References
-
- Berbari EF, Kanj SS, Kowalski TJ, Darouiche RO, Widmer AF, Schmitt SK, et al. Executive summary: 2015 infectious diseases society of America (IDSA) Clinical Practice Guidelines for the Diagnosis and Treatment of Native Vertebral Osteomyelitis in Adults. Clin Infect Dis. (2015) 61:859–63. 10.1093/cid/civ633 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials