

Case Report: Management of a Patient With Chylomicronemia Syndrome During Pregnancy With Medical Nutrition Therapy
- PMID: 33748172
- PMCID: PMC7973004
- DOI: 10.3389/fnut.2021.602938
Case Report: Management of a Patient With Chylomicronemia Syndrome During Pregnancy With Medical Nutrition Therapy
Abstract
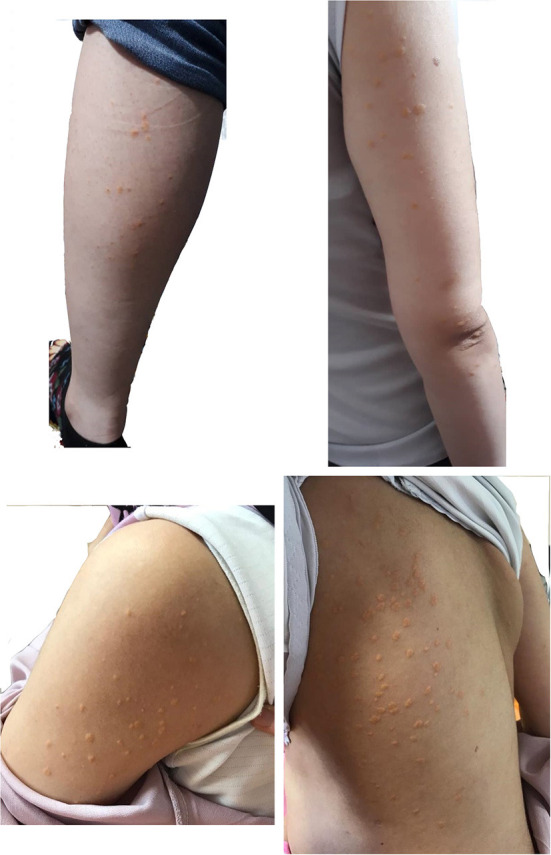
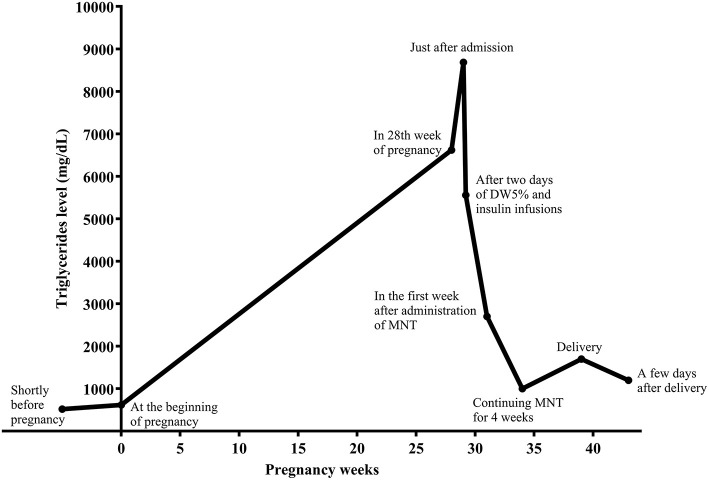
Background: Hypertriglyceridemia (HTG) during pregnancy may be accompanied by acute pancreatitis, hyperviscosity syndrome, and preeclampsia. HTG during pregnancy should be managed by a multidisciplinary team; however, no clinical guidelines exist for severe gestational HTG. Case Presentation: We herein present a case of a 36-year-old in the first pregnancy (G1P0Ab0), with a history of severe HTG-induced necrotizing pancreatitis 9 years earlier. There was no family history of HTG. During these years, she did not follow any appropriate diet or medical therapy for HTG. She became pregnant in May 2019, without preconception counseling. Eruptive and tuberoeruptive xanthomas appeared in the 27th week of pregnancy. Serum triglycerides (TGs) and fasting blood sugar (FBS) were 6,620 and 124 mg/dL, respectively, indicating HTG and gestational diabetes (GDM). After admission for the management of severe HTG, she was put on parenteral nutrition with dextrose water 5% and infusion insulin therapy without receiving any enteral carbohydrate for 2 days. Following that, a very low-fat diet and omega-3 fatty acids (1,200 mg/day) were started. After 4 weeks, TG levels reached 1,000 mg/dL, and her self-monitoring blood glucose levels showed appropriate blood glucose for pregnancy. She underwent a successful elective cesarean section in the 39th of pregnancy. Conclusion: This case report demonstrates that HTG during pregnancy could be managed by medical nutrition therapy (MNT).
Keywords: GDM; chylomicronemia syndrome; hypertriglyceridemia; medical nutrition therapy; pregnant women.
Copyright © 2021 Zahedi, Asghari, Mirmiran and Hosseinpanah.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Recurrent Pancreatitis in a Pregnant Woman with Severe Hypertriglyceridemia Successfully Managed by Multiple Plasmapheresis.J Atheroscler Thromb. 2022 Jul 1;29(7):1108-1116. doi: 10.5551/jat.62734. Epub 2021 Jul 2. J Atheroscler Thromb. 2022. PMID: 34219115 Free PMC article.
-
Management of Severe Hypertriglyceridemia in Pregnancy With Niacin: Reevaluating Safety and Therapeutic Benefits.Case Rep Endocrinol. 2025 Jan 30;2025:2644678. doi: 10.1155/crie/2644678. eCollection 2025. Case Rep Endocrinol. 2025. PMID: 39949380 Free PMC article.
-
Acute Pancreatitis in the Transgender Population.Cureus. 2021 Jul 3;13(7):e16140. doi: 10.7759/cureus.16140. eCollection 2021 Jul. Cureus. 2021. PMID: 34277301 Free PMC article.
-
Hospital Management of Severe Hypertriglyceridemia in Children.Curr Pediatr Rev. 2017;13(4):225-231. doi: 10.2174/1573400514666180117092707. Curr Pediatr Rev. 2017. PMID: 29345595 Review.
-
Current knowledge of hypertriglyceridemic pancreatitis.Eur J Intern Med. 2014 Oct;25(8):689-94. doi: 10.1016/j.ejim.2014.08.008. Epub 2014 Sep 27. Eur J Intern Med. 2014. PMID: 25269432 Review.
Cited by
-
Multidisciplinary diagnosis and treatment of severe acute pancreatitis associated with hypertriglyceridemia in pregnancy: a case report.Ann Transl Med. 2022 Aug;10(16):911. doi: 10.21037/atm-22-3313. Ann Transl Med. 2022. PMID: 36111044 Free PMC article.
-
Brazilian Position Statement for Familial Chylomicronemia Syndrome - 2023.Arq Bras Cardiol. 2023 Mar;120(4):e20230203. doi: 10.36660/abc.20230203. Arq Bras Cardiol. 2023. PMID: 37075362 Free PMC article. English, Portuguese. No abstract available.
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous