

Bedside cardiopulmonary ultrasonography evaluates lung water content in very low-weight preterm neonates with patent ductus arteriosus
- PMID: 33748231
- PMCID: PMC7953406
- DOI: 10.12998/wjcc.v9.i8.1827
Bedside cardiopulmonary ultrasonography evaluates lung water content in very low-weight preterm neonates with patent ductus arteriosus
Abstract
Background: Patent ductus arteriosus (PDA) is a common congenital heart abnormality in preterm neonates with a high incidence in neonates with very low birth weights. When PDA persists, interstitial lung water content increases, which could lead to abnormal circulation hemodynamics and pulmonary edema. It is important to perform early and reliable assessment of lung water content in very low-weight preterm neonates with persistent PDA.
Aim: To evaluate the role of bedside cardiopulmonary ultrasonography in the lung water content assessment in very low-weight preterm neonates with persistent PDA.
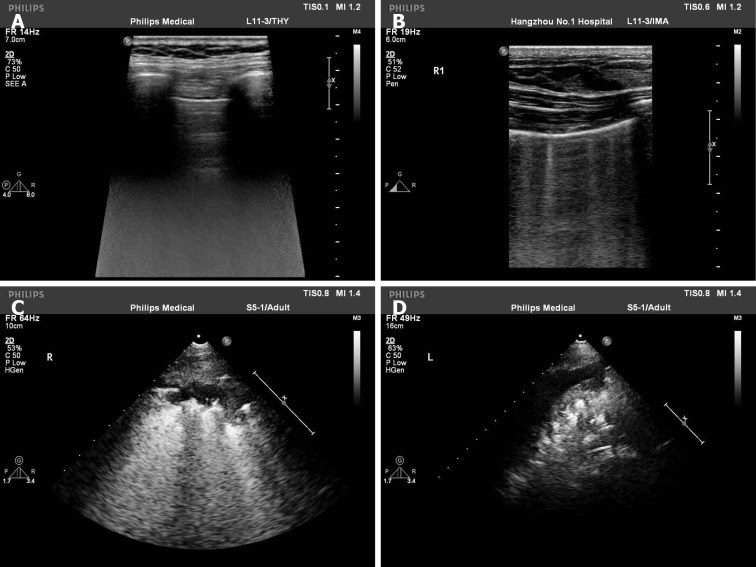
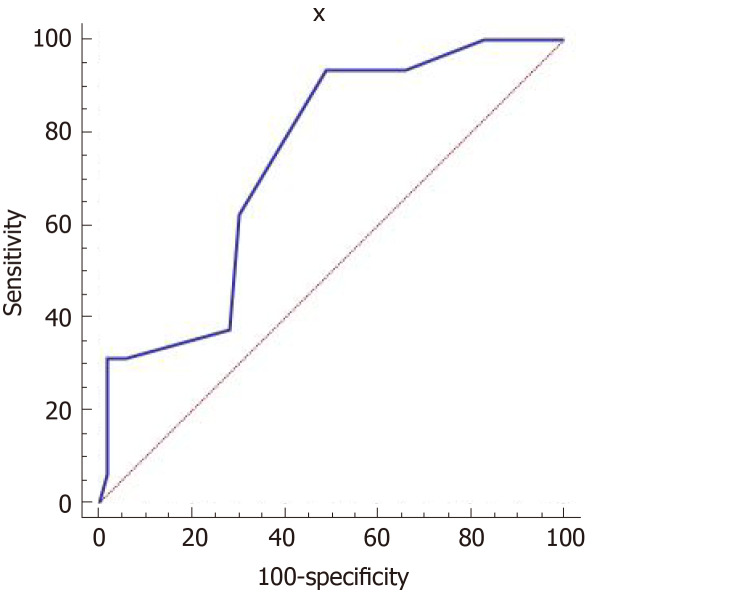
Methods: From January 2018 to March 2020, 69 very low-weight preterm neonates with echocardiography-confirmed PDA were selected as the PDA group. At the same time, 89 very low-weight preterm neonates without PDA were randomly selected as the control group. All neonates underwent echocardiography and 6-segment lung ultrasonography on the fourth day after birth. The clinical characteristics and main ultrasonography results were compared between the two groups. Pearson's analysis was used to analyze the correlation between lung ultrasonography score (LUS) and other related clinical and ultrasonography results in all neonates. In the PDA group, PDA diameters were recorded, and the correlation with LUS and left atrium to aortic (LA/AO) dimension ratio were also analyzed. LA/AO ratio is one of the ultrasonic diagnostic criteria for hemodynamically significant PDA. When the ratio is ≥ 1.5, it suggests the possibility of hemodynamic changes in persistent PDA. A receiver operating characteristic curve was established using the sensitivity of LUS to predict the hemodynamic changes in neonates with PDA as the ordinate and 1-specificity as the abscissa.
Results: A total of 158 neonates were enrolled in this study, including 69 in the PDA group and 89 in the control group. There were no statistical differences in sex, gestational age, birth weight, ventilator dependence, hospitalization length and left ventricular ejection fraction between the two groups (P > 0.05). The LUS and LA/AO ratio in the PDA group were higher than those in the control group (P < 0.05), but there was no difference of LUS in neonates with or without use of the ventilator (t = 0.58, P = 0.16). In all cases, LUS was negatively correlated with gestational age (r = -0.28, P < 0.01) and birth weight (r = -0.36, P < 0.01), while positively correlated with the LA/AO ratio (r = 0.27, P < 0.01). In the PDA group, PDA diameter was positively correlated with the LA/AO ratio (r = 0.39, P < 0.01) and LUS (r = 0.31, P < 0.01). Receiver operating characteristic results showed that LUS had the moderate accuracy for predicting hemodynamic changes in PDA (area under the curve = 0.741; sensitivity = 93.75%; specificity = 50.94%).
Conclusion: Bedside cardiopulmonary ultrasonography can evaluate lung content in neonates with PDA and predict the possibility of hemodynamic changes in persistent PDA.
Keywords: Cardiopulmonary; Lung ultrasound score; Patent ductus arteriosus; Preterm; Ultrasonography; Very low-weight neonates.
©The Author(s) 2021. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: There are no conflicts of interest to report.
Figures
References
-
- Sekar KC. Protective strategies to prevent patent ductus arteriosus. Chin Med J (Engl) . 2010;123:2914–2918. - PubMed
-
- Zhang L, Shen W, Chen C, Pan JH. Clinical analysis of risk factors and complications of HSPDA in premature infants. Zhonghua Quanke Yixue Zazhi . 2019;8:1299–1301.
-
- Kluckow M, Evans N. Ductal shunting, high pulmonary blood flow, and pulmonary hemorrhage. J Pediatr . 2000;137:68–72. - PubMed
-
- Saldeño YP, Favareto V, Mirpuri J. Prolonged persistent patent ductus arteriosus: potential perdurable anomalies in premature infants. J Perinatol . 2012;32:953–958. - PubMed
-
- Kurepa D, Zaghloul N, Watkins L, Liu J. Neonatal lung ultrasound exam guidelines. J Perinatol . 2018;38:11–22. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
