

Laryngopharyngeal reflux disease management for recurrent laryngeal contact granuloma: A case report
- PMID: 33748251
- PMCID: PMC7953387
- DOI: 10.12998/wjcc.v9.i8.1989
Laryngopharyngeal reflux disease management for recurrent laryngeal contact granuloma: A case report
Abstract
Background: Laryngeal contact granuloma (LCG) is difficult to treat and frequently associated with high persistence and recurrence, despite the availability of both surgical and pharmacological treatment options. An appropriate strategy is therefore needed to help patients with multiple recurrences of LCG to potentially avoid unnecess-ary surgery.
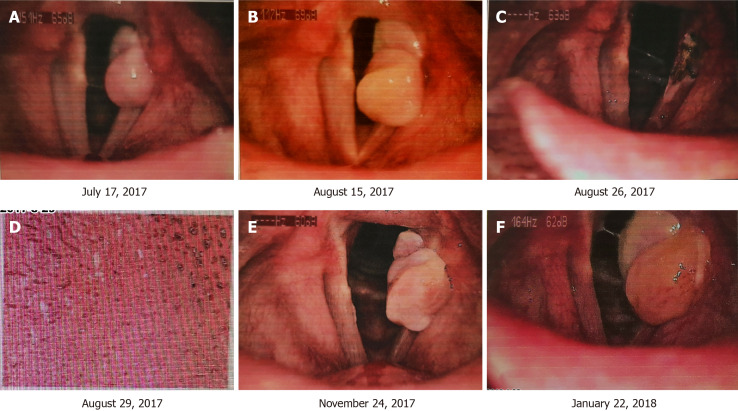
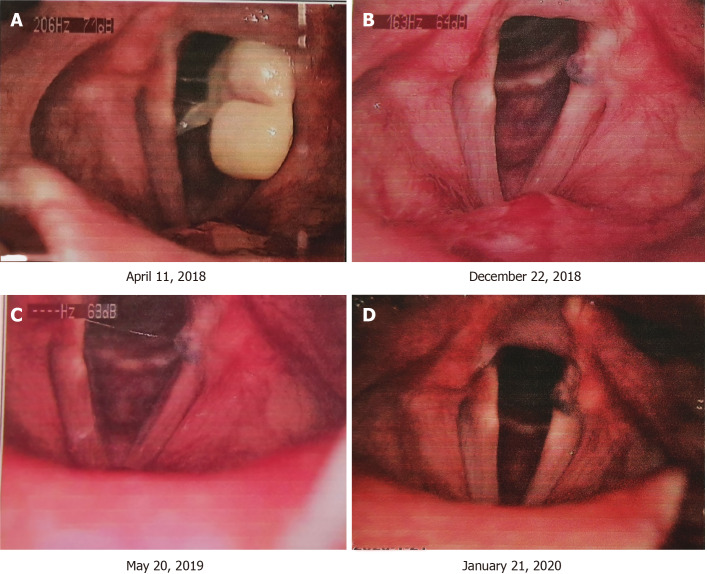
Case summary: We describe the case of a 34-year-old male patient with recurrent LCG in which a good response was achieved through successful management of laryngophar-yngeal reflux disease using a combination pharmacotherapeutic regimen consisting of anti-reflux therapy, pepsin secretion inhibition, bile acid neutralization, and lifestyle modifications. This patient underwent surgery to excise the granuloma, then relapsed, underwent a second surgery, which was followed by a second recurrence. The granuloma then disappeared after 9 mo of combined treatment with ilaprazole enteric-coated capsules (10 mg qd), mosapride tablets (5 mg tid) and compound digestive enzyme capsules (2 tablets). The drug regimen was discontinued after one year, and no recurrence of the lesion has been reported during the one-year follow-up period.
Conclusion: We report a combination of pharmacotherapeutics and lifestyle modifications for the management of laryngopharyngeal reflux disease to address recurring LCG.
Keywords: Anti-reflux therapy; Bile acid neutralization; Case report; Laryngopharyngeal reflux disease management; Pepsin secretion inhibition; Recurrent laryngeal contact granuloma.
©The Author(s) 2021. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors have no funding, financial relationships, or conflicts of interest to disclose.
Figures

Similar articles
-
Noninvasive Detection of Arytenoid Cartilage Calcification Using Computed Tomography and Prediction of Prognosis in Laryngeal Contact Granuloma.J Voice. 2024 Mar;38(2):466-471. doi: 10.1016/j.jvoice.2021.09.003. Epub 2021 Oct 8. J Voice. 2024. PMID: 34629228
-
[Relationship between laryngopharyngeal reflux and calcification of arytenoid cartilage in male patients with idiopathic laryngeal contact granuloma].Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2020 Mar;34(3):263-265. doi: 10.13201/j.issn.2096-7993.2020.03.019. Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2020. PMID: 32791597 Free PMC article. Chinese.
-
A management strategy for vocal process granulomas.Laryngoscope. 1999 Feb;109(2 Pt 1):301-6. doi: 10.1097/00005537-199902000-00023. Laryngoscope. 1999. PMID: 10890783
-
Diagnosis and management of laryngopharyngeal reflux disease.Curr Opin Otolaryngol Head Neck Surg. 2006 Jun;14(3):150-5. doi: 10.1097/01.moo.0000193177.62074.fd. Curr Opin Otolaryngol Head Neck Surg. 2006. PMID: 16728891 Review.
-
[Current status of treatment of laryngeal contact granuloma].Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2017 Aug 5;31(15):1217-1220. doi: 10.13201/j.issn.1001-1781.2017.15.020. Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2017. PMID: 29798364 Review. Chinese.
Cited by
-
The effectiveness of various treatment approaches for laryngeal contact granulomas.Eur Arch Otorhinolaryngol. 2024 Apr;281(4):1877-1884. doi: 10.1007/s00405-023-08436-5. Epub 2024 Jan 11. Eur Arch Otorhinolaryngol. 2024. PMID: 38206391
References
-
- Carroll TL, Gartner-Schmidt J, Statham MM, Rosen CA. Vocal process granuloma and glottal insufficiency: an overlooked etiology? Laryngoscope. 2010;120:114–120. - PubMed
-
- Chen M, Chen J, Yang Y, Li CJ, Wu HT, Chen L. Conservative Treatment versus Surgery for Laryngeal Contact Granuloma: A Prospective Study. ORL J Otorhinolaryngol Relat Spec. 2018;80:307–316. - PubMed
-
- Ylitalo R, Lindestad PA. Laryngeal findings in patients with contact granuloma: a long-term follow-up study. Acta Otolaryngol. 2000;120:655–659. - PubMed
-
- al-Dousary S. Vocal process granuloma. Ear Nose Throat J. 1997;76:382–386, 387. - PubMed
-
- Chang W, Xu W, Cheng L. Treatment of Laryngeal Contact Granuloma: Surgical Therapy or Conservative Treatment. ORL J Otorhinolaryngol Relat Spec. 2019;81:348–353. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
