

Interrater and Intrarater Reliability and Discriminant Validity of a Pediatric Lower Extremity Physical Therapy Clearance Test
- PMID: 33748298
- PMCID: PMC7938390
- DOI: 10.1177/2325967120983827
Interrater and Intrarater Reliability and Discriminant Validity of a Pediatric Lower Extremity Physical Therapy Clearance Test
Abstract
Background: Few studies have validated when an athlete can safely return to sports, and even fewer have identified when he or she no longer requires physical therapy after surgery. Discontinuing physical therapy is often dictated by insurance restrictions, but most studies have suggested that the decision should be multifactorial, stemming from patient-derived subjective outcome questionnaires, clinical examination, and isokinetic and functional testing.
Purpose/hypothesis: The purpose of this study was to establish discriminant validity and reliability of an objective physical therapy clearance (PTC) test in a clinical setting. The hypotheses were that the PTC test (1) will demonstrate different scores between normal and postoperative cohorts and (2) will have acceptable inter- and intraobserver reliability.
Study design: Cohort study (diagnosis); Level of evidence, 3.
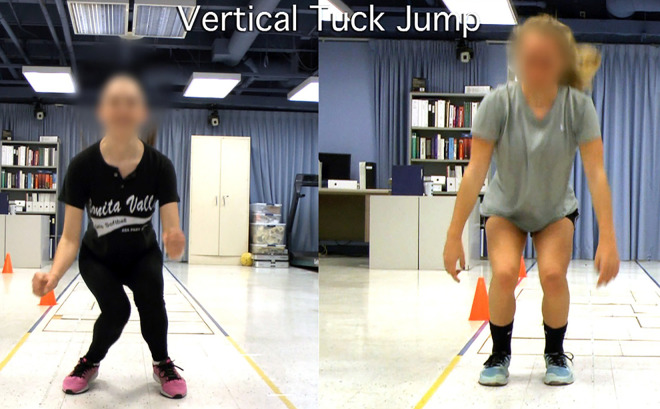
Methods: Four cohorts (27 total participants; age range, 12-18 years) underwent the PTC test: 9 adolescents 6 months after anterior cruciate ligament reconstruction, 4 adolescents 6 weeks after partial meniscectomy, 5 adolescents with nonstructural knee pain, and 9 control/healthy participants without any lower extremity complaint. The PTC test included a dynamic warm-up, objective measures (knee range of motion, thigh girth, and muscle motor tone), functional strength tests (heel raises, single-leg dips, hop tests, tuck jumps), and agility tests (shuffle and sprint T-test). Each testing session was videotaped and scored live by the physical therapist administering the test, and then scored via the video recording by an independent physical therapist and 2 orthopaedic surgeons.
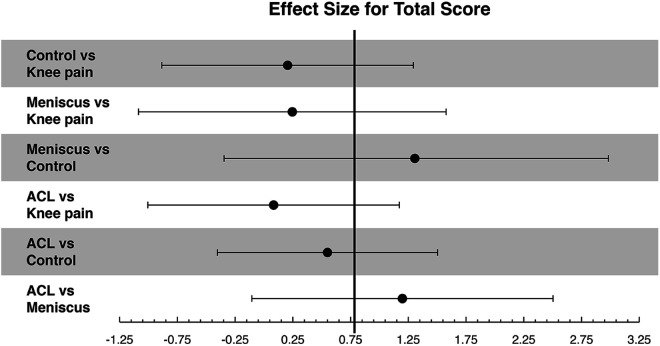
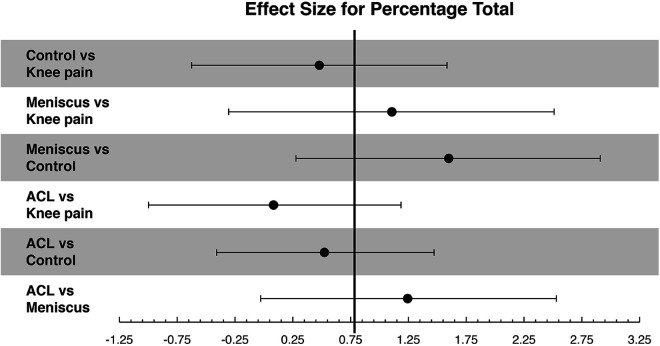
Results: The PTC test was found to have discriminant validity between the control cohort and both cohorts with previous surgery. The single-leg dip, single-leg hop, and vertical tuck jump were the most discriminatory components. The PTC test had moderate to almost perfect intrarater reliability (κ = 0.57-1), but only fair to moderate interrater reliability among video graders (κ = 0.29-0.58) and slight to substantial reliability between video graders and the live PT rater (κ = 0.19-0.63).
Conclusion: The PTC test was found to have moderate inter- and intraobserver agreement, with the ability to discriminate between postoperative and control patients.
Keywords: adolescent; functional test; pediatric; physical therapy; return to sport.
© The Author(s) 2021.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: M.D.E. has received educational support from Arthrex. A.T.P. has received educational support from Sportstek Medical, consulting fees from OrthoPediatrics, and nonconsulting fees from Smith & Nephew and has stock/stock options in Imagen. E.W.E. has received consulting fees from OrthoPediatrics and nonconsulting fees from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures
Similar articles
-
INTER AND INTRA-RATER RELIABILITY OF THE DROP VERTICAL JUMP (DVJ) ASSESSMENT.Int J Sports Phys Ther. 2020 Oct;15(5):770-775. doi: 10.26603/ijspt20200770. Int J Sports Phys Ther. 2020. PMID: 33110696 Free PMC article.
-
Report of the Clinical and Functional Primary Outcomes in Men of the ACL-SPORTS Trial: Similar Outcomes in Men Receiving Secondary Prevention With and Without Perturbation Training 1 and 2 Years After ACL Reconstruction.Clin Orthop Relat Res. 2017 Oct;475(10):2523-2534. doi: 10.1007/s11999-017-5280-2. Clin Orthop Relat Res. 2017. PMID: 28224443 Free PMC article. Clinical Trial.
-
QUANTIFYING FRONTAL PLANE KNEE KINEMATICS IN SUBJECTS WITH ANTERIOR KNEE PAIN: THE RELIABILITY AND CONCURRENT VALIDITY OF 2D MOTION ANALYSIS.Int J Sports Phys Ther. 2018 Feb;13(1):86-93. Int J Sports Phys Ther. 2018. PMID: 29484245 Free PMC article.
-
A Critically Appraised Topic on the Tuck Jump Assessment: Does the Tuck Jump Assessment Demonstrate Interrater and Intrarater Reliability in Healthy Individuals?J Sport Rehabil. 2019 Oct 16;29(4):503-508. doi: 10.1123/jsr.2019-0099. Print 2020 May 1. J Sport Rehabil. 2019. PMID: 31624223 Review.
-
Association between Functional Performance and Return to Performance in High-Impact Sports after Lower Extremity Injury: A Systematic Review.J Sports Sci Med. 2020 Aug 13;19(3):564-576. eCollection 2020 Sep. J Sports Sci Med. 2020. PMID: 32874110 Free PMC article.
Cited by
-
Unique Considerations for the Pediatric Athlete During Rehabilitation and Return to Sport After Anterior Cruciate Ligament Reconstruction.Arthrosc Sports Med Rehabil. 2022 Jan 28;4(1):e221-e230. doi: 10.1016/j.asmr.2021.09.037. eCollection 2022 Jan. Arthrosc Sports Med Rehabil. 2022. PMID: 35141555 Free PMC article.
References
-
- Barber-Westin SD, Noyes FR. Factors used to determine return to unrestricted sports activities after anterior cruciate ligament reconstruction. Arthroscopy. 2011;27(12):1697–1705. - PubMed
-
- Bohannon RW. Measuring knee extensor muscle strength. Am J Phys Med Rehabil. 2001;80(1):13–18. - PubMed
-
- Chang EW, Johnson S, Pollard C, Hoffman M, Norcross M. Landing biomechanics in anterior cruciate ligament reconstructed females who pass or fail a functional test battery. Knee. 2018;25(6):1074–1082. - PubMed
-
- Ekstrom RA, Donatelli RA, Carp KC. Electromyographic analysis of core trunk, hip, and thigh muscles during 9 rehabilitation exercises. J Orthop Sports Phys Ther. 2007;37(12):754–762. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
