

Clinical Outcomes, Survivorship, and Return to Sport After Arthroscopic Capsular Repair With Suture Anchors for Adolescent Multidirectional Shoulder Instability: Results at 6-Year Follow-up
- PMID: 33748302
- PMCID: PMC7903833
- DOI: 10.1177/2325967121993879
Clinical Outcomes, Survivorship, and Return to Sport After Arthroscopic Capsular Repair With Suture Anchors for Adolescent Multidirectional Shoulder Instability: Results at 6-Year Follow-up
Abstract
Background: Multidirectional shoulder instability (MDI) refractory to rehabilitation can be treated with arthroscopic capsulolabral reconstruction with suture anchors. To the best of our knowledge, no studies have reported on outcomes or examined the risk factors that contribute to poor outcomes in adolescent athletes.
Purpose: To identify risk factors for surgical failure by comparing anatomic, clinical, and demographic variables in adolescents who underwent intervention for MDI.
Study design: Case series; Level of evidence, 4.
Methods: All patients 20 years or younger who underwent arthroscopic shoulder surgery at a single institution between January 2009 and April 2017 were evaluated. MDI was defined by positive drive-through sign on arthroscopy plus positive sulcus sign and/or multidirectional laxity on anterior and posterior drawer tests while under anesthesia. A 2-year minimum follow-up was required, but those whose treatment failed earlier were also included. Demographic characteristics and intraoperative findings were recorded, as were scores on the Single Assessment Numeric Evaluation (SANE), Pediatric and Adolescent Shoulder Survey (PASS), and short version of the Disabilities of the Arm, Shoulder and Hand (QuickDASH).
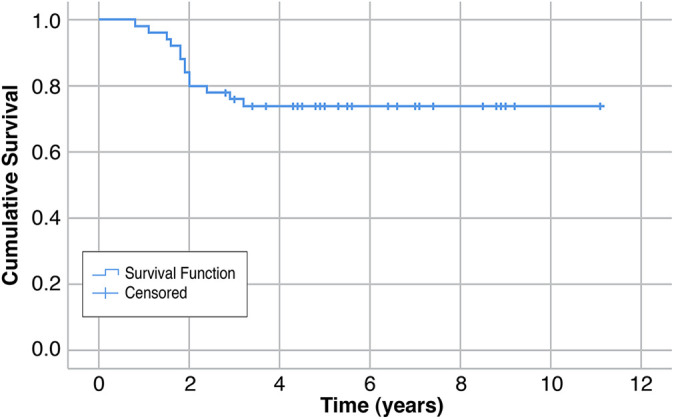
Results: Overall, 42 adolescents (50 shoulders; 31 female, 19 male) were identified as having undergone surgical treatment for MDI with minimum 2-year follow-up or failure. The mean follow-up period was 6.3 years (range, 2.8-10.2 years). Surgical failure, defined as recurrence of subluxation and instability, was noted in 13 (26.0%) shoulders; all underwent reoperation at a mean of 1.9 years (range, 0.8-3.2 years). None of the anatomic, clinical, or demographic variables tested, or the presence of generalized ligamentous laxity, was associated with subjective outcomes or reoperation. Number of anchors used was not different between shoulders that failed and those that did not fail. Patients reported a mean SANE score of 83.3, PASS score of 85.0, and QuickDASH score of 6.8. Return to prior level of sport occurred in 56% of patients.
Conclusion: Adolescent MDI refractory to nonsurgical management appeared to have long-term outcomes after surgical intervention that were comparable with outcomes of adolescent patients with unidirectional instability. In patients who experienced failure of capsulorrhaphy, results showed that failure most likely occurred within 3 years of the index surgical treatment.
Keywords: anterior shoulder; glenoid labrum; multidirectional instability; pediatric and adolescent; posterior shoulder.
© The Author(s) 2021.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: B.C.M. and M.Y.S. have received education payments from SportsTek Medical. A.T.P. has received education payments from Arthrex and SportsTek Medical, consulting fees from OrthoPediatrics, and speaking fees from Smith & Nephew, and he has stock/stock options in Imagen. E.W.E. has received consulting fees from OrthoPediatrics and speaking fees from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures
References
-
- Altchek DW, Warren RF, Skyhar MJ, Ortiz G. T-plasty modification of the Bankart procedure for multidirectional instability of the anterior and inferior types. J Bone Joint Surg Am. 1991;73(1):105–112. - PubMed
-
- Asturias AM, Bastrom TP, Pennock AT, Edmonds EW. Posterior shoulder instability: surgical outcomes and risk of failure in adolescence. Am J Sports Med. 2020;48(5):1200–1206. - PubMed
-
- Bak K, Spring BJ, Henderson JP. Inferior capsular shift procedure in athletes with multidirectional instability based on isolated capsular and ligamentous redundancy. Am J Sports Med. 2000;28(4):466–471. - PubMed
-
- Baker CL, Mascarenhas R, Kline AJ, Chhabra A, Pombo MW, Bradley JP. Arthroscopic treatment of multidirectional shoulder instability in athletes: a retrospective analysis of 2- to 5-year clinical outcomes. Am J Sports Med. 2009;37(9):1712–1720. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
