

Infectious necrotizing scleritis and proliferative vitreoretinopathy after scleral buckling in a patient with atopic dermatitis
- PMID: 33748537
- PMCID: PMC7966824
- DOI: 10.1016/j.ajoc.2021.101066
Infectious necrotizing scleritis and proliferative vitreoretinopathy after scleral buckling in a patient with atopic dermatitis
Abstract
Purpose: To report a case of necrotizing scleritis and proliferative vitreoretinopathy due to an acute infection following scleral buckling for the management of rhegmatogenous retinal detachment in a patient with untreated atopic dermatitis.
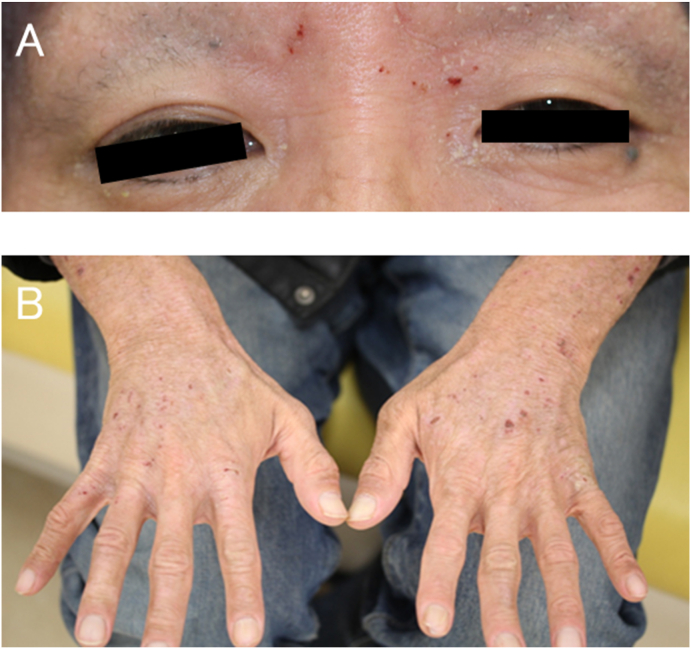
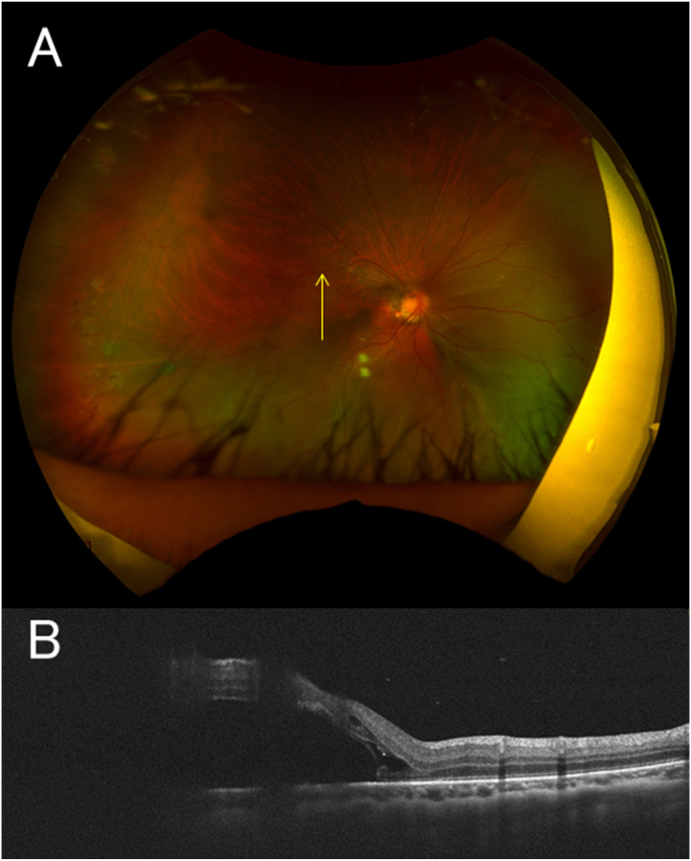
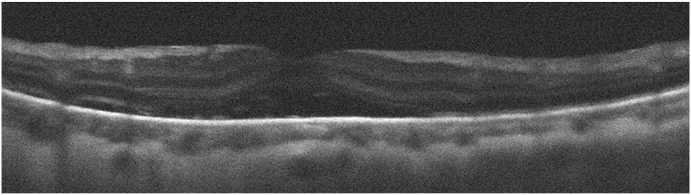
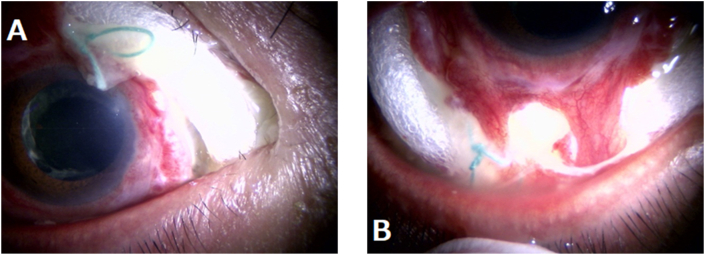
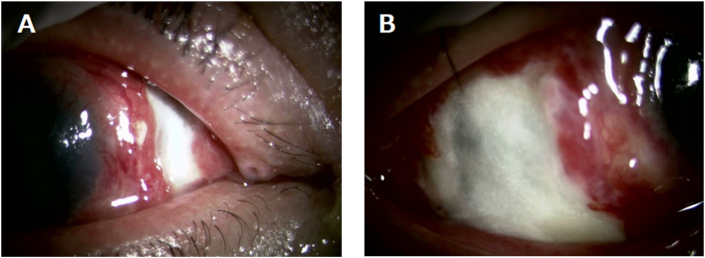
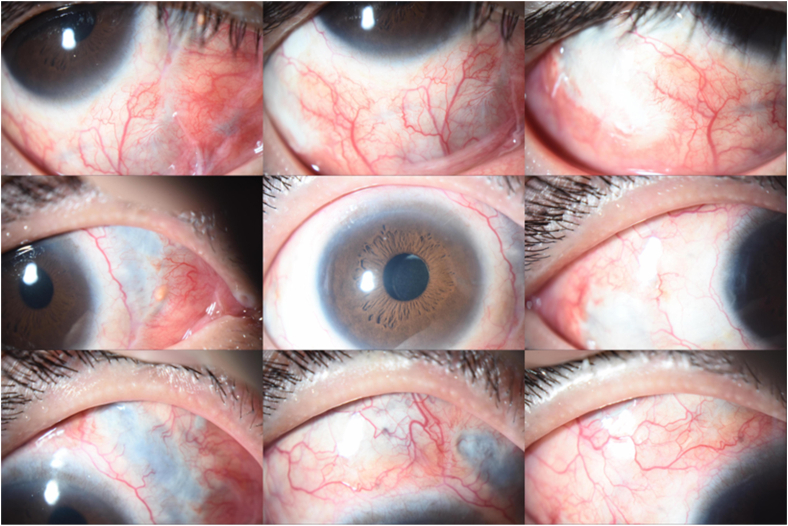
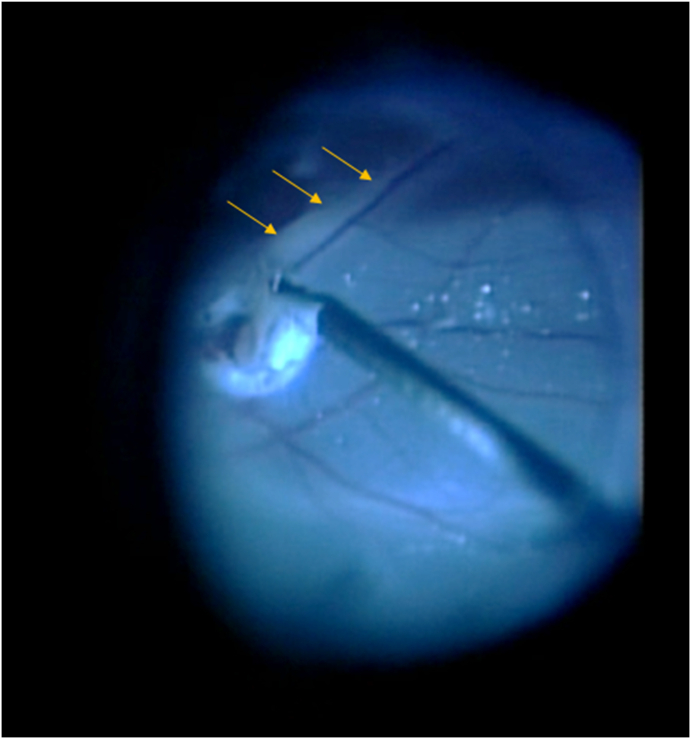
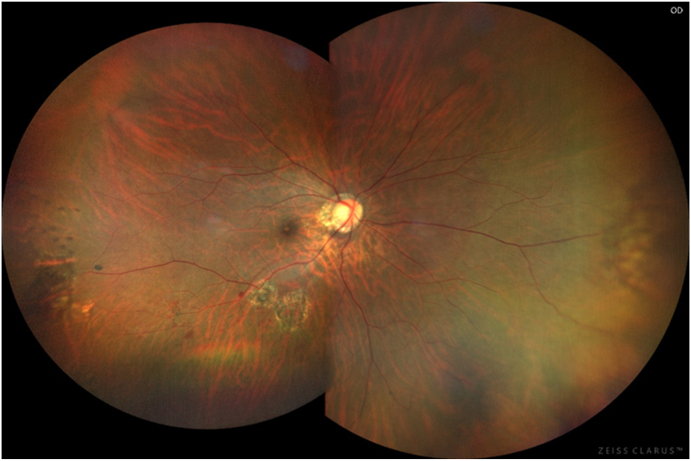
Observations: A 40-year-old man with untreated atopic dermatitis presented with rhegmatogenous retinal detachment in his right eye. He underwent uncomplicated scleral buckling surgery with an encircling silicon sponge band, then noticed severe hyperemia and purulent discharge in the eye at 3 weeks after surgery. The silicon sponge was exposed and had migrated anteriorly. The patient was then diagnosed with post-scleral-buckling infection and underwent scleral buckle removal. Marked scleral thinning due to necrotizing scleritis was evident beneath the scleral buckle. Eye discharge culture findings were positive for Staphylococcus aureus. After removal of the scleral buckle, the patient's necrotizing scleritis improved, but he developed proliferative vitreoretinopathy. The patient then underwent pars plana vitrectomy, which resulted in reattachment of his retina.
Conclusions and importance: Although postoperative infection within 1 month after scleral buckling is rare, surgeons should note that patients with atopic dermatitis are at high risk of postoperative infection after scleral buckling, leading to the development of sight-threatening complications such as necrotizing scleritis, which could lead to incomplete retinal attachment and proliferative vitreoretinopathy.
Keywords: Atopic dermatitis; Necrotizing scleritis; Pars plana vitrectomy; Postoperative infection; Retinal detachment; Scleral buckling.
© 2021 The Authors.
Conflict of interest statement
The following authors have no financial disclosures; (H.S, Y.H, T.H, Y.K).
Figures
References
-
- Lincoff H.A., Baras I., McLEAN J. Modifications to the custodis procedure for retinal detachment. Arch Ophthalmol. 1965;73(2):160–163. - PubMed
-
- Machemer R., Buettner H., Norton E.W., Parel J.M. Vitrectomy: a pars plana approach. Trans Am Acad Ophthalmol Otolaryngol. 1971;75(4):813–820. - PubMed
-
- Eckardt C. Transconjunctival sutureless 23-gauge vitrectomy. Retina. 2005;25(2):208–211. - PubMed
-
- O'Malley C., Heintz R.M. Vitrectomy with an alternative instrument system. Ann Ophthalmol. 1975;7(4):585–594. - PubMed
-
- Storey P., Alshareef R., Khuthaila M. Pars plana vitrectomy and scleral buckle versus pars plana vitrectomy alone for patients with rhegmatogenous retinal detachment at high risk for proliferative vitreoretinopathy. Retina. 2014;34(10):1945–1951. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
