

Determining C5, C6 and C7 myotomes through comparative analyses of clinical, MRI and EMG findings in cervical radiculopathy
- PMID: 33748550
- PMCID: PMC7966958
- DOI: 10.1016/j.cnp.2021.02.002
Determining C5, C6 and C7 myotomes through comparative analyses of clinical, MRI and EMG findings in cervical radiculopathy
Abstract
Objective: There are many myotome charts in the literature, but few studies have presented actual data to support their identification. We aimed to determine C5/C6/C7 myotomes based on clinical and EMG data of patients with cervical spondylotic radiculopathy (CSR) having a single-root lesion confirmed by MRI.
Methods: Medical Research Council (MRC) scores and EMG findings were retrospectively reviewed for patients enrolled from our EMG database.
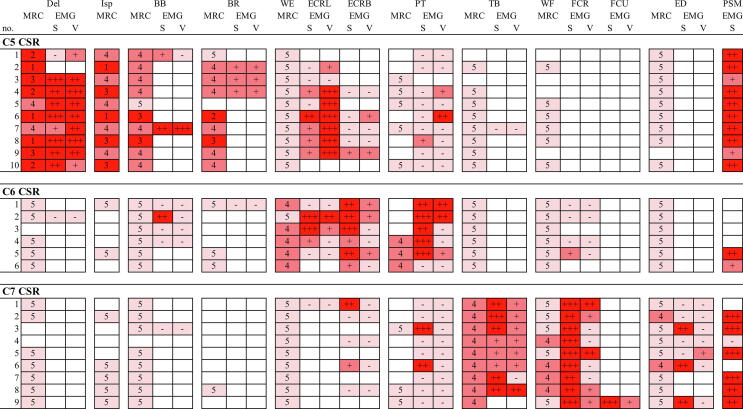
Results: Enrolled were 25 patients (10 C5, 6 C6, and 9 C7 CSR). In C5 CSR, weakness or denervation potentials in EMG, or both, were observed in the deltoid (Del) and infraspinatus (Isp) muscles for all patients, and in the biceps brachii (BB) and brachioradialis (BR) muscles for 9/10 and 8/9 patients, respectively. In C6 CSR, weakness of the wrist extensor and/or denervation of the extensor carpi radialis longus (ECRL)/extensor carpi radialis brevis (ECRB), and those of the pronator teres (PT) were observed for all patients. Weakness was not observed for any other muscle in C6 CSR. Denervation potentials of ECRL were found in 5/8 and 3/5 patients with C5 and C6 CSR, respectively, whereas those of ECRB were found in 1/5, 6/6, and 2/5 patients with C5, C6 and C7 CSR, respectively. In C7 CSR, weakness/denervation of the triceps brachii (TB) and denervation potentials of the flexor carpi radialis (FCR) were observed for all patients. Denervation potentials in PT and weakness/denervation of the extensor digitorum (ED) were observed in 2/9 and 4/9 patients, respectively.
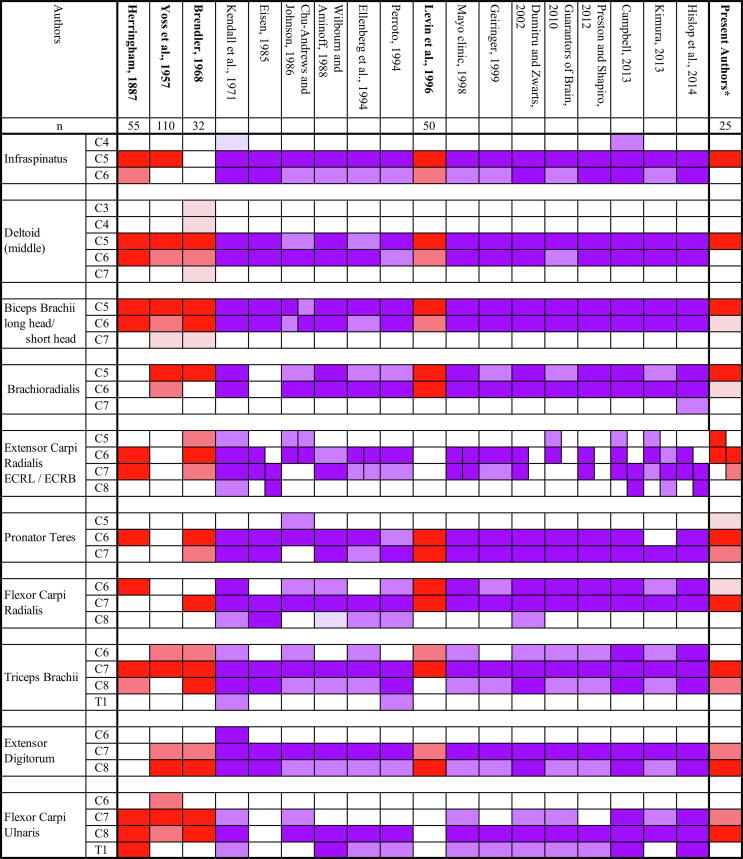
Conclusion: Suggested dominant myotomes are: C5 for the Del, Isp, BB, and BR, C5/6 for the ECRL, C6 > C7 for the ECRB and PT, and C7 for the TB and FCR.
Significance: The current study identified dominant myotomes that differ from the existing literature.
Keywords: Brachioradialis; Cervical spondylotic radiculopathy; Extensor carpi radialis brevis; Extensor carpi radialis longus; Myotome; Pronator teres.
© 2021 International Federation of Clinical Neurophysiology. Published by Elsevier B.V.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- American Association of Electrodiagnostic Medicine Guidelines in electrodiagnostic medicine. Practice parameter for needle electromyographic evaluation of patients with suspected cervical radiculopathy. Muscle Nerve Suppl. 1999;8:S209–S221. - PubMed
-
- Brendler S.J. The human cervical myotomes: functional anatomy studied at operation. J. Neurosurg. 1968;28:105–111. - PubMed
-
- Campbell W.W. 7th ed. Wolters Kluwer; Philadelphia: 2013. Dejong's the Neurologic Examination.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
