

NAFLD and MAFLD as emerging causes of HCC: A populational study
- PMID: 33748726
- PMCID: PMC7957147
- DOI: 10.1016/j.jhepr.2021.100231
NAFLD and MAFLD as emerging causes of HCC: A populational study
Abstract
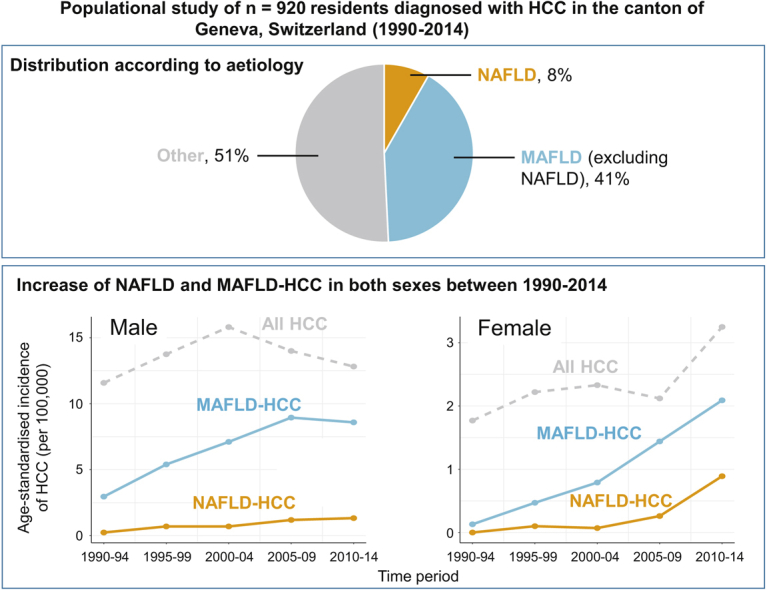
Background & aims: There are conflicting data regarding the epidemiology of hepatocellular carcinoma (HCC) arising in the context of non-alcoholic and metabolic-associated fatty liver disease (NAFLD and MAFLD). We aimed to examine the changing contribution of NAFLD and MAFLD, stratified by sex, in a well-defined geographical area and highly characterised HCC population between 1990 and 2014.
Methods: We identified all patients with HCC resident in the canton of Geneva, Switzerland, diagnosed between 1990 and 2014 from the prospective Geneva Cancer Registry and assessed aetiology-specific age-standardised incidence. NAFLD-HCC was diagnosed when other causes of liver disease were excluded in cases with type 2 diabetes, metabolic syndrome, or obesity. Criteria for MAFLD included one or more of the following criteria: overweight/obesity, presence of type 2 diabetes mellitus, or evidence of metabolic dysregulation.
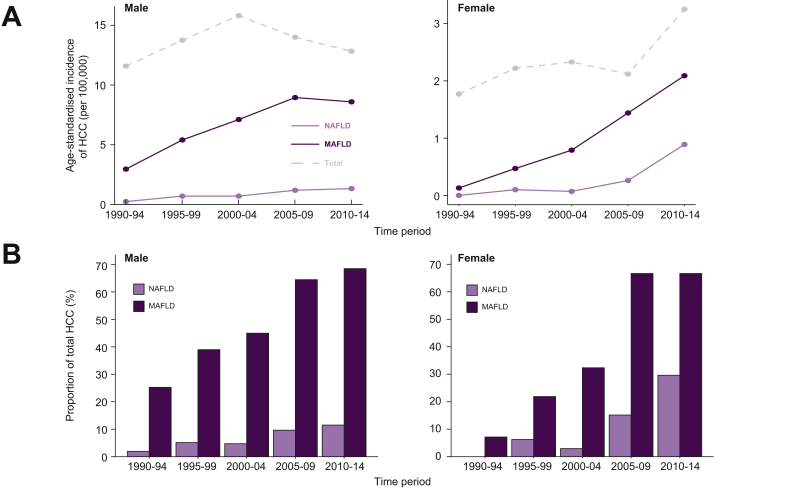
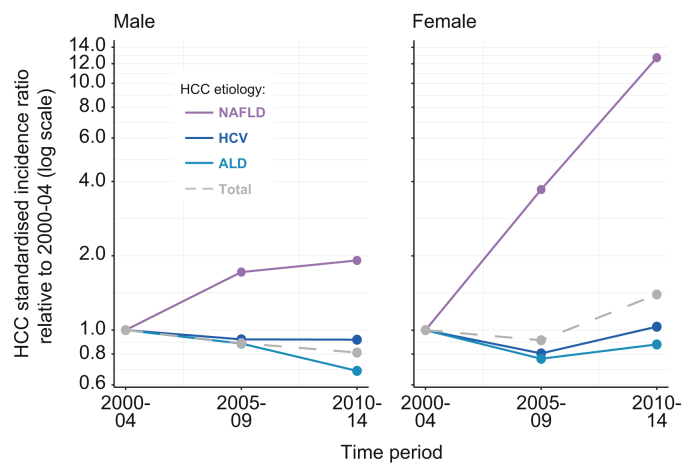
Results: A total of 76/920 (8.3%) of patients were diagnosed with NAFLD-HCC in the canton of Geneva between 1990 and 2014. Between the time periods 1990-1994 and 2010-2014, there was a significant increase in HCC incidence in women (standardised incidence ratio [SIR] 1.83, 95% CI 1.08-3.13, p = 0.026) but not in men (SIR 1.10, 95% CI 0.85-1.43, p = 0.468). In the same timeframe, the proportion of NAFLD-HCC increased more in women (0-29%, p = 0.037) than in men (2-12%, p = 0.010) while the proportion of MAFLD increased from 21% to 68% in both sexes and from 7% to 67% in women (p <0.001). From 2000-2004 to 2010-2014, the SIR of NAFLD-HCC increased to 1.92 (95% CI 0.77-5.08) for men and 12.7 (95% CI 1.63-545) in women, whereas it decreased or remained stable for other major aetiologies of HCC.
Conclusions: In a populational cohort spanning 25 years, the burden of NAFLD and MAFLD associated HCCs increased significantly, driving an increase in HCC incidence, particularly in women.
Lay summary: Hepatocellular carcinoma (HCC) is the most common type of liver cancer, increasingly arising in patients with liver disease caused by metabolic syndrome, termed non-alcoholic fatty liver disease (NAFLD) or metabolic-associated fatty liver disease (MAFLD). We assessed all patients with HCC between 1990 and 2014 in the canton of Geneva (western Switzerland) and found an increase in all HCC cases in this timeframe, particularly in women. In addition, we found that HCC caused by NAFLD or MAFLD significantly increased over the years, particularly in women, possibly driving the increase in overall HCC cases.
Keywords: AFP, alpha-foetoprotein; ALD, alcohol-related liver disease; ALT, alanine transaminase; ASI, age-standardised incidence; AST, aspartate aminotransferase; Fatty liver; GGT, gamma-glutamyltransferase; HCC, hepatocellular carcinoma; HR, hazard ratio; Hepatocellular carcinoma; INR, international normalised ratio; Liver cancer; MAFLD, metabolic-associated fatty liver disease; MELD, model for end-stage liver disease; Metabolic syndrome; NAFLD, non-alcoholic fatty liver disease; SIR, standardised incidence ratio; TACE, transarterial chemoembolisation; Women’s health.
© 2021 The Author(s).
Conflict of interest statement
The authors declare no conflicts of interest that pertain to this work. Please refer to the accompanying ICMJE disclosure forms for further details.
Figures
References
-
- Bray F., Ferlay J., Soerjomataram I., Siegel R.L., Torre L.A., Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Canc J Clin. 2018;68:394–424. - PubMed
-
- Howlader N., Noone A., Krapcho M., Miller D., Bishop K., Kosary C. National Cancer Institute; Bethesda, MD: 2017. SEER Cancer Statistics Review, 1975–2014; pp. 1–12.
-
- Liu Z., Jiang Y., Yuan H., Fang Q., Cai N., Suo C. The trends in incidence of primary liver cancer caused by specific etiologies: results from the Global Burden of Disease Study 2016 and implications for liver cancer prevention. J Hepatol. 2019;70:674–683. - PubMed
-
- Zhang X., El-Serag H.B., Thrift A.P. Sex and race disparities in the incidence of hepatocellular carcinoma in the United States examined through age–period–cohort analysis. Canc Epidemiol Biomarkers Prev. 2020;29:88–94. - PubMed
-
- Younossi Z.M., Koenig A.B., Abdelatif D., Fazel Y., Henry L., Wymer M. Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology. 2016;64:73–84. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
