

The effect of remote ischaemic conditioning on blood pressure response: A systematic review and meta-analysis
- PMID: 33748739
- PMCID: PMC7972960
- DOI: 10.1016/j.ijchy.2021.100081
The effect of remote ischaemic conditioning on blood pressure response: A systematic review and meta-analysis
Abstract
Background: Previous work has evaluated the effect of remote ischaemic conditioning (RIC) in a number of clinical conditions (e.g. cardiac surgery and acute kidney injury), but only one analysis has examined blood pressure (BP) changes. While individual studies have reported the effects of acute bouts and repeated RIC exposure on resting BP, efficacy is equivocal. We conducted a systematic review and meta-analysis to evaluate the effects of acute and repeat RIC on BP.
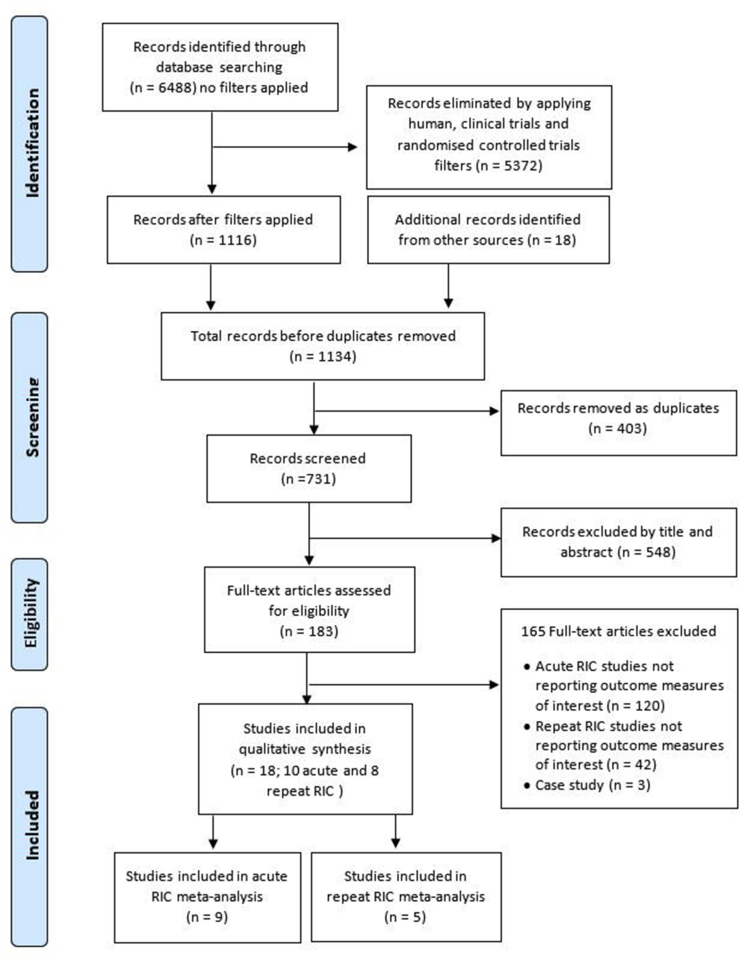
Methods: A systematic search was performed using PubMed, Web of Science, EMBASE, and Cochrane Library of Controlled Trials up until October 31, 2020. Additionally, manual searches of reference lists were performed. Studies that compared BP responses after exposing participants to either an acute bout or repeated cycles of RIC with a minimum one-week intervention period were considered.
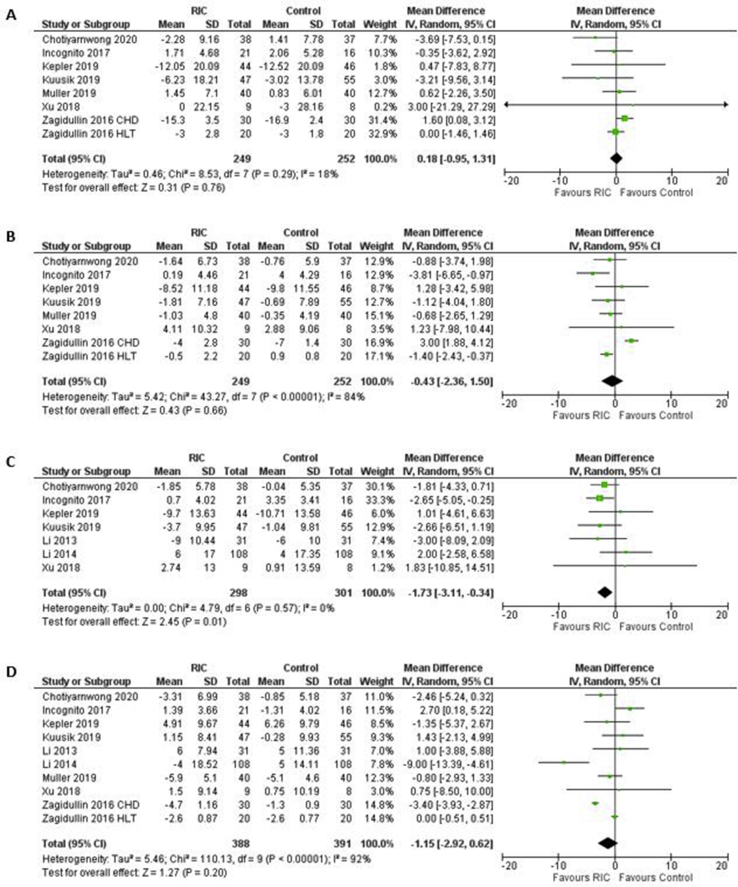
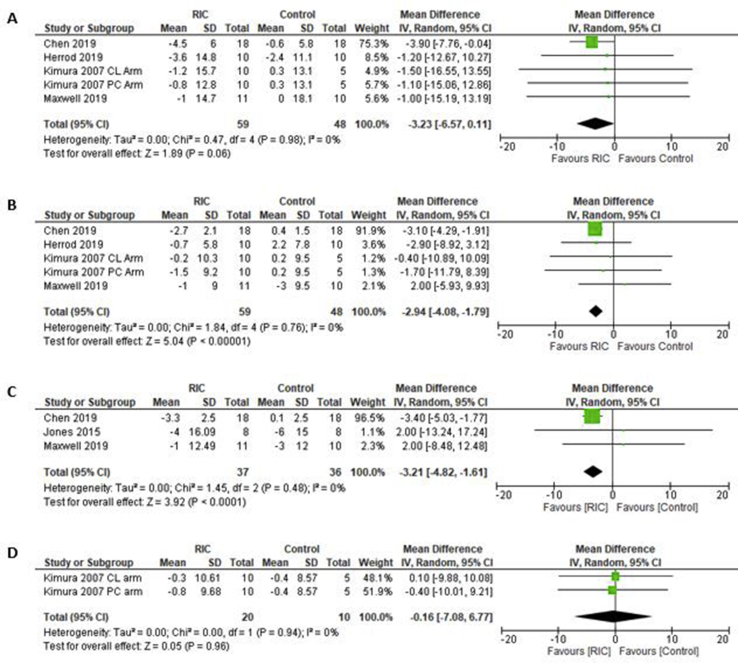
Results: Eighteen studies were included in this systematic review, ten examined acute effects while eight investigated repeat effects of RIC. Mean differences (MD) for outcome measures from acute RIC studies were: systolic BP 0.18 mmHg (95%CI -0.95, 1.31; p = 0.76), diastolic BP -0.43 mmHg (95%CI -2.36, 1.50; p = 0.66), MAP -1.73 mmHg (95%CI -3.11, -0.34; p = 0.01) and HR -1.15 bpm (95%CI -2.92, 0.62; p = 0.20). Only MAP was significantly reduced. Repeat RIC exposure showed non-significant change in systolic BP -3.23 mmHg (95%CI -6.57, 0.11; p = 0.06) and HR -0.16 bpm (95%CI -7.08, 6.77; p = 0.96) while diastolic BP -2.94 mmHg (95%CI -4.08, -1.79; p < 0.00001) and MAP -3.21 mmHg (95%CI -4.82, -1.61; p < 0.0001) were significantly reduced.
Conclusions: Our data suggests repeated, but not acute, RIC produced clinically meaningful reductions in diastolic BP and MAP.
Keywords: Acute remote ischaemic conditioning; BP, blood pressure; Blood pressure; CABG, coronary artery bypass grafting; CI, confidence interval; HR, heart rate; MD, mean difference; RIC; RIC, Remote ischaemic conditioning; Repeat remote ischaemic conditioning; SD, standard deviation; T2DM, type 2 diabetes mellitus; VEGF, vascular endothelial growth factor.
© 2021 Published by Elsevier B.V.
Conflict of interest statement
None of the authors declare any conflicts of interest.
Figures
References
-
- GBD 2017 Causes of Death Collaborators Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1736–1788. doi: 10.1016/s0140-6736(18)32203-7. - DOI - PMC - PubMed
-
- Whelton P.K., Carey R.M., Aronow W.S., Casey D.E., Collins K.J., Himmelfarb C.D., DePalma S.M., Gidding S., Jamerson K.A., Jones D.W. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults. A report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. J. Am. Coll. Cardiol. 2018;71(19):e127–e248. doi: 10.1016/j.jacc.2017.11.006. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
