

SGLT2i versus ARNI in heart failure with reduced ejection fraction: a systematic review and meta-analysis
- PMID: 33749159
- PMCID: PMC8120387
- DOI: 10.1002/ehf2.13313
SGLT2i versus ARNI in heart failure with reduced ejection fraction: a systematic review and meta-analysis
Abstract
Aims: This study aimed to determine the effects of sodium-glucose cotransporter-2 inhibitor (SGLT2i) in heart failure with reduced ejection fraction (HFrEF), compare the effect of SGLT2i with angiotensin receptor neprilysin inhibitor (ARNI), and find whether combination of SGLT2i and ARNI is better than monotherapy.
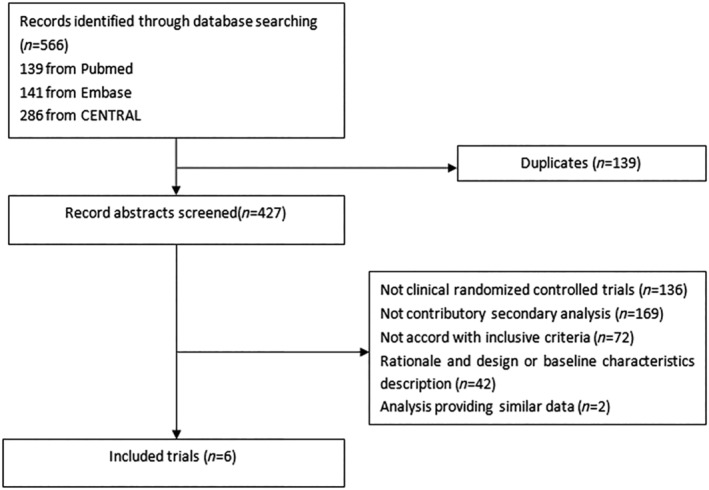
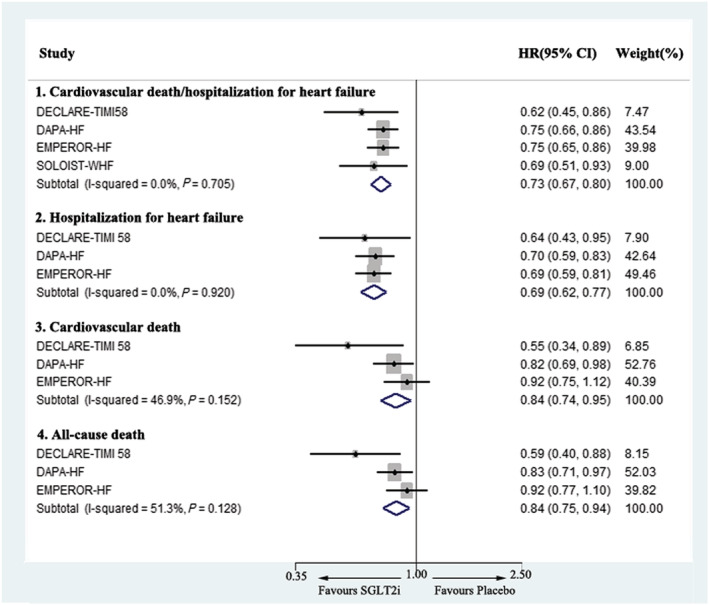
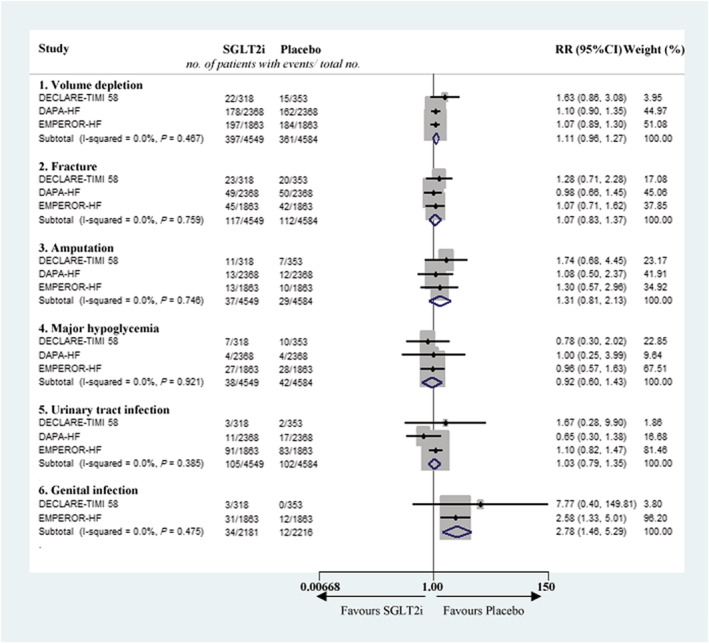
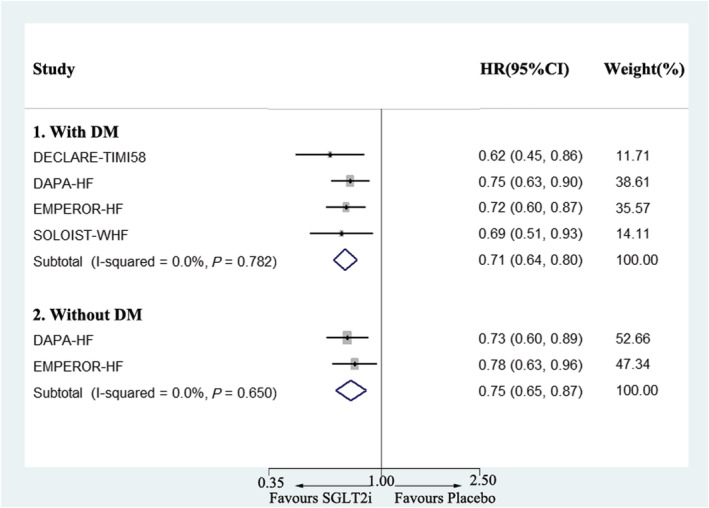
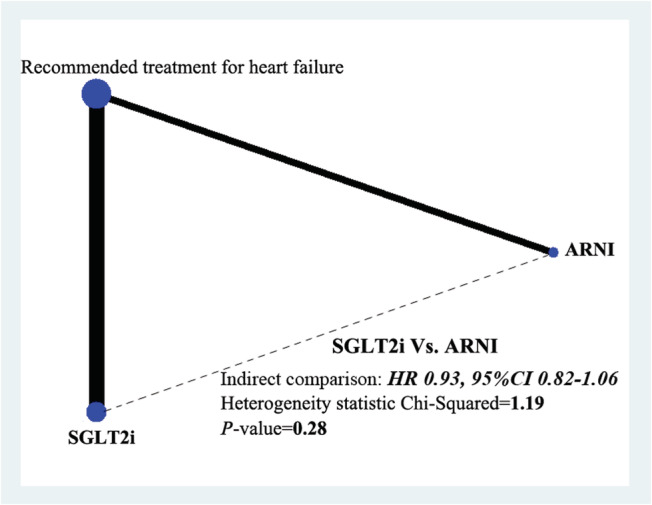
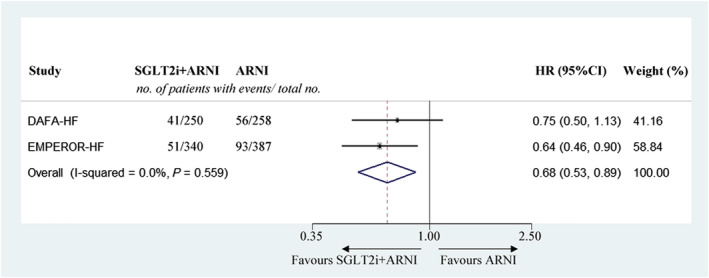
Methods and results: Embase, Medline, and Cochrane Central Registry of Controlled Trials were searched for randomized controlled trials evaluating SGLT2i or ARNI in HFrEF. And a total of six trials were included. SGLT2i was found to significantly reduce the risk of cardiovascular death or hospitalization for heart failure by 27% [hazard ratio (HR) 0.73, 95% confidence interval (CI) 0.67-0.80], hospitalization for heart failure by 31% (HR 0.69, 95% CI 0.62-0.77), cardiovascular death by 16% (HR 0.84, 95% CI 0.74-0.95), and all-cause death by 16% (HR 0.84, 95% CI 0.75-0.94) in HFrEF only with a statistically higher risk of genital infection (risk ratio (RR) 2.78, 95% CI 1.46-5.29). The reduction in cardiovascular death or hospitalization for heart failure was of similar magnitude in patients with or without diabetes mellitus (HR 0.71, 95% CI 0.64-0.80 vs. HR 0.75, 95% CI 0.65-0.87) using SGLT2i. Indirect treatment comparison showed that SGLT2i and ARNI had similar effects on primary outcome (HR 0.93, 95% CI 0.82-1.06). And combination of SGLT2i and ARNI achieved a better prognosis performance (HR 0.68, 95% CI 0.53-0.89) compared with ARNI monotherapy.
Conclusions: SGLT2i could safely reduce cardiovascular death or hospitalization for heart failure in HFrEF regardless of diabetes mellitus status. SGLT2i and ARNI demonstrate similar effects, while combination of SGLT2i and ARNI results in a better cardiovascular protective effect.
Keywords: Angiotensin receptor neprilysin inhibitor; Heart failure with reduced ejection fraction; Meta-analysis; Sodium-glucose cotransporter-2 inhibitor.
© 2021 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
Yuling Yan, Bin Liu, Jun Du, Jing Wang, Xiaodong Jing, Yajie Liu, Songbai Deng, Jianlin Du, and Qiang She declare that they have no conflict of interest.
Figures
References
-
- Lee HY, Baek SH. Optimal use of beta‐blockers for congestive heart failure. Circ J 2016; 80: 565–571. - PubMed
-
- Nochioka K, Sakata Y, Shimokawa H. Combination therapy of renin angiotensin system inhibitors and β‐blockers in patients with heart failure. Adv Exp Med Biol 2018; 1067: 17–30. - PubMed
-
- Chia N, Fulcher J, Keech A. Beta‐blocker, angiotensin‐converting enzyme inhibitor/angiotensin receptor blocker, nitrate‐hydralazine, diuretics, aldosterone antagonist, ivabradine, devices and digoxin (BANDAID2): an evidence‐based mnemonic for the treatment of systolic heart failure. Intern Med J 2016; 46: 653–662. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical