

Applying Clinical Decision Support Design Best Practices With the Practical Robust Implementation and Sustainability Model Versus Reliance on Commercially Available Clinical Decision Support Tools: Randomized Controlled Trial
- PMID: 33749610
- PMCID: PMC8077777
- DOI: 10.2196/24359
Applying Clinical Decision Support Design Best Practices With the Practical Robust Implementation and Sustainability Model Versus Reliance on Commercially Available Clinical Decision Support Tools: Randomized Controlled Trial
Abstract
Background: Limited consideration of clinical decision support (CDS) design best practices, such as a user-centered design, is often cited as a key barrier to CDS adoption and effectiveness. The application of CDS best practices is resource intensive; thus, institutions often rely on commercially available CDS tools that are created to meet the generalized needs of many institutions and are not user centered. Beyond resource availability, insufficient guidance on how to address key aspects of implementation, such as contextual factors, may also limit the application of CDS best practices. An implementation science (IS) framework could provide needed guidance and increase the reproducibility of CDS implementations.
Objective: This study aims to compare the effectiveness of an enhanced CDS tool informed by CDS best practices and an IS framework with a generic, commercially available CDS tool.
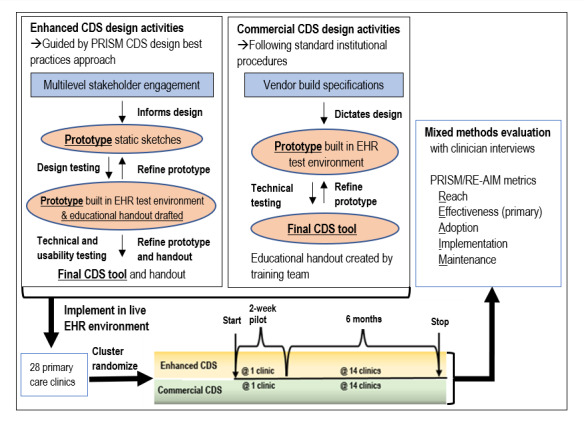
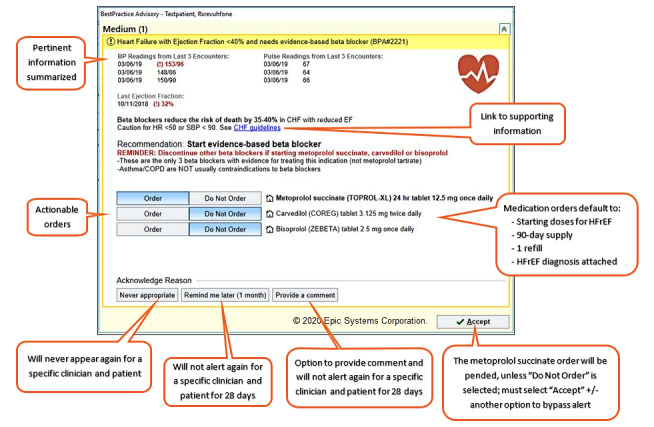
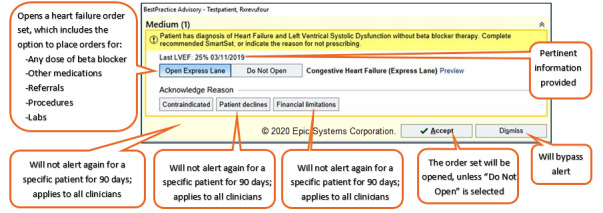
Methods: We conducted an explanatory sequential mixed methods study. An IS-enhanced and commercial CDS alert were compared in a cluster randomized trial across 28 primary care clinics. Both alerts aimed to improve beta-blocker prescribing for heart failure. The enhanced alert was informed by CDS best practices and the Practical, Robust, Implementation, and Sustainability Model (PRISM) IS framework, whereas the commercial alert followed vendor-supplied specifications. Following PRISM, the enhanced alert was informed by iterative, multilevel stakeholder input and the dynamic interactions of the internal and external environment. Outcomes aligned with PRISM's evaluation measures, including patient reach, clinician adoption, and changes in prescribing behavior. Clinicians exposed to each alert were interviewed to identify design features that might influence adoption. The interviews were analyzed using a thematic approach.
Results: Between March 15 and August 23, 2019, the enhanced alert fired for 61 patients (106 alerts, 87 clinicians) and the commercial alert fired for 26 patients (59 alerts, 31 clinicians). The adoption and effectiveness of the enhanced alert were significantly higher than those of the commercial alert (62% vs 29% alerts adopted, P<.001; 14% vs 0% changed prescribing, P=.006). Of the 21 clinicians interviewed, most stated that they preferred the enhanced alert.
Conclusions: The results of this study suggest that applying CDS best practices with an IS framework to create CDS tools improves implementation success compared with a commercially available tool.
Trial registration: ClinicalTrials.gov NCT04028557; http://clinicaltrials.gov/ct2/show/NCT04028557.
Keywords: PRISM; RE-AIM; clinical decision support systems; congestive heart failure; implementation science.
©Katy E Trinkley, Miranda E Kroehl, Michael G Kahn, Larry A Allen, Tellen D Bennett, Gary Hale, Heather Haugen, Simeon Heckman, David P Kao, Janet Kim, Daniel M Matlock, Daniel C Malone, Robert L Page 2nd, Jessica Stine, Krithika Suresh, Lauren Wells, Chen-Tan Lin. Originally published in JMIR Medical Informatics (http://medinform.jmir.org), 22.03.2021.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Bates DW, Kuperman GJ, Wang S, Gandhi T, Kittler A, Volk L, Spurr C, Khorasani R, Tanasijevic M, Middleton B. Ten commandments for effective clinical decision support: making the practice of evidence-based medicine a reality. J Am Med Inform Assoc. 2003 Nov 1;10(6):523–30. doi: 10.1197/jamia.m1370. - DOI - PMC - PubMed
-
- Osheroff J, Teich J, Levick D, Saldana L, Velasco F, Sittig D. Improving Outcomes With Clinical Decision Support: an Implementers Guide. Chicago, IL: Healthcare Information Management Systems Society (HIMSS); 2012.
-
- Horsky J, Schiff GD, Johnston D, Mercincavage L, Bell D, Middleton B. Interface design principles for usable decision support: a targeted review of best practices for clinical prescribing interventions. J Biomed Inform. 2012 Dec;45(6):1202–16. doi: 10.1016/j.jbi.2012.09.002. https://linkinghub.elsevier.com/retrieve/pii/S1532-0464(12)00149-9 - DOI - PubMed
-
- Sittig DF, Wright A, Osheroff JA, Middleton B, Teich JM, Ash JS, Campbell E, Bates DW. Grand challenges in clinical decision support. J Biomed Inform. 2008 Apr;41(2):387–92. doi: 10.1016/j.jbi.2007.09.003. http://linkinghub.elsevier.com/retrieve/pii/S1532-0464(07)00104-9 - DOI - PMC - PubMed
-
- Shah N, Seger A, Seger D, Fiskio J, Kuperman G, Blumenfeld B, Recklet E, Bates D, Gandhi T. Improving acceptance of computerized prescribing alerts in ambulatory care. J Am Med Inform Assoc. 2006;13(1):5–11. doi: 10.1197/jamia.M1868. http://europepmc.org/abstract/MED/16221941 - DOI - PMC - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
