

Inclusion of Synovial Tissue-Derived Characteristics in a Nomogram for the Prediction of Treatment Response in Treatment-Naive Rheumatoid Arthritis Patients
- PMID: 33750008
- PMCID: PMC8457106
- DOI: 10.1002/art.41726
Inclusion of Synovial Tissue-Derived Characteristics in a Nomogram for the Prediction of Treatment Response in Treatment-Naive Rheumatoid Arthritis Patients
Abstract
Objective: This study applied a synovitis score obtained during routine care from ultrasound (US)-guided biopsies of synovial tissue (ST) in patients with rheumatoid arthritis (RA) and patients with other inflammatory and noninflammatory joint diseases to identify pretreatment synovial biomarkers associated with disease characteristics, and to integrate the findings into a multiparameter nomogram for use in baseline prediction of diagnosis and treatment response in treatment-naive rheumatoid arthritis (RA) patients.
Methods: The study enrolled a total of 1,015 patients with various autoimmune diseases (545 patients with RA, 167 patients with psoriatic arthritis [PsA], 199 patients with undifferentiated peripheral inflammatory arthritis [UPIA], 18 patients with crystal-induced arthritis, 26 patients with connective tissue diseases, and 60 patients with osteoarthritis [OA] [as part of the SYNGem cohort]). All patients underwent a US-guided ST biopsy at baseline, and patients were then stratified according to disease phase. The KSS, along with disease characteristics and clinical outcomes, were incorporated into a nomogram for prediction of achievement of clinical remission in RA patients who were previously naive to treatment. In patients in whom a treat-to-target strategy was applied, remission was defined as change in the Disease Activity Score in 28 joints (DAS28) at 6 months after treatment initiation.
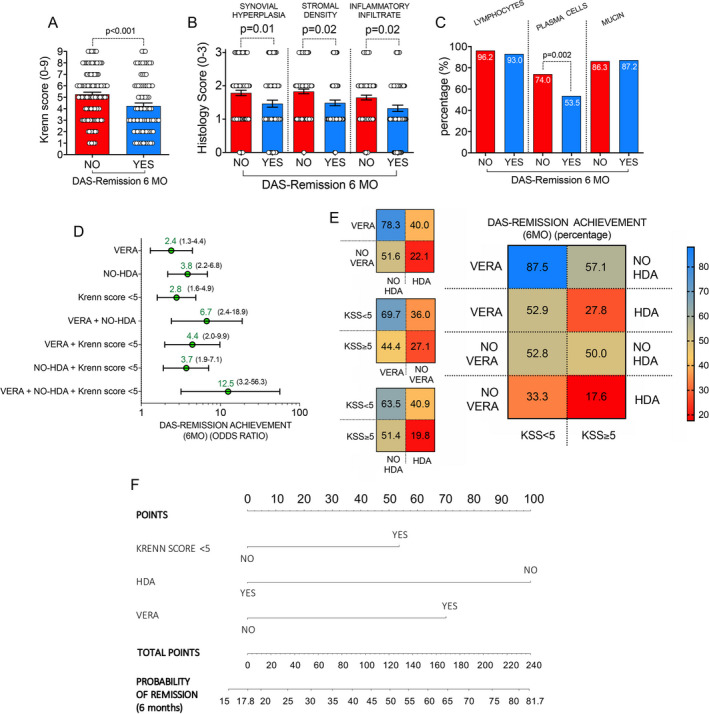
Results: The KSS significantly differed among RA patients, as well as PsA patients and UPIA patients, when compared to OA patients. In RA, the KSS directly correlated with the DAS28 and was related to autoantibody positivity in treatment-naive RA patients. Moreover, at baseline, treatment-naive RA patients achieving 6-month remission according to DAS28 had a lower KSS, shorter duration of symptoms (very early RA [VERA]), and lower disease activity than treatment-naive RA patients not achieving remission according to DAS28. Results of logistic regression analysis identified the following synergistic predictive factors of achievement of DAS28-based disease remission at 6 months: having a short disease duration (VERA), not having high disease activity, and having a KSS of <5 at baseline. A nomogram integrating these baseline clinical and histologic characteristics in treatment-naive RA patients yielded an up to 81.7% probability of achieving 6-month remission according to the DAS28.
Conclusion: The KSS is a reliable tool for synovitis assessment on US-guided ST biopsy, contingent on the phase of the disease and the autoimmune profile of each patient. This tool could be integrated within a therapeutic response-predictive nomogram for the prediction of treatment response in RA patients who were previously naive to treatment.
© 2021 The Authors. Arthritis & Rheumatology published by Wiley Periodicals LLC on behalf of American College of Rheumatology.
Figures




References
-
- Lliso‐Ribera G, Humby F, Lewis M, Nerviani A, Mauro D, Rivellese F, et al. Synovial tissue signatures enhance clinical classification and prognostic/treatment response algorithms in early inflammatory arthritis and predict requirement for subsequent biological therapy: results from the pathobiology of early arthritis cohort (PEAC). Ann Rheum Dis 2019;78:1642–52. - PMC - PubMed
-
- Smolen JS, Landewé R, Bijlsma J, Burmester GR, Dougados M, Kerschbaumer A, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease‐modifying antirheumatic drugs: 2019 update. Ann Rheum Dis 2020;79:685–99. - PubMed
-
- Krenn V, Morawietz L, Burmester GR, Kinne RW, Mueller‐Ladner U, Muller B, et al. Synovitis score: discrimination between chronic low‐grade and high‐grade synovitis. Histopathology 2006;49:358–64. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
