

Evaluation of microscopy, serology, circulating anodic antigen (CAA), and eosinophil counts for the follow-up of migrants with chronic schistosomiasis: a prospective cohort study
- PMID: 33750443
- PMCID: PMC7941883
- DOI: 10.1186/s13071-021-04655-z
Evaluation of microscopy, serology, circulating anodic antigen (CAA), and eosinophil counts for the follow-up of migrants with chronic schistosomiasis: a prospective cohort study
Abstract
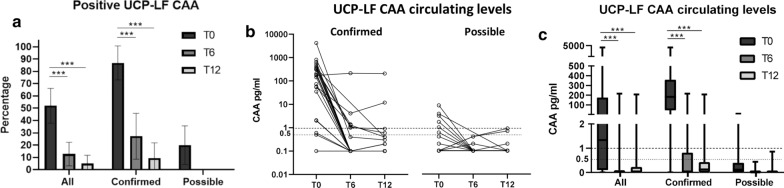
Background: An accurate test for the diagnosis and post-treatment follow-up of patients with schistosomiasis is needed. We assessed the performance of different laboratory parameters, including the up-converting reporter particle technology lateral flow assay to detect circulating anodic antigen (UCP-LF CAA), for the post-treatment follow-up of schistosomiasis in migrants attending a dedicated outpatient clinic in a non-endemic country.
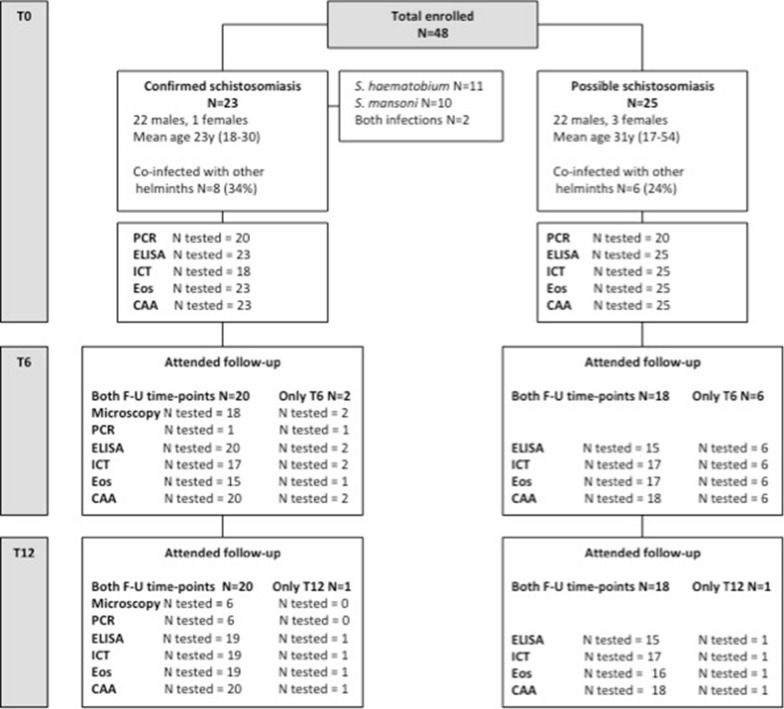
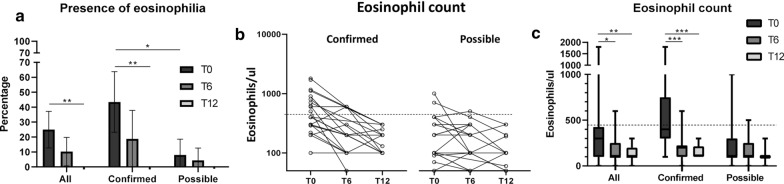
Methods: Routine anti-Schistosoma serology results and eosinophil counts were obtained of patients with positive urine/stool microscopy and/or PCR (confirmed cases) or only positive serology (possible cases), and at least one follow-up visit at 6 (T6) or 12 (T12) months after praziquantel treatment. All sera samples were tested with the UCP-LF CAA assay.
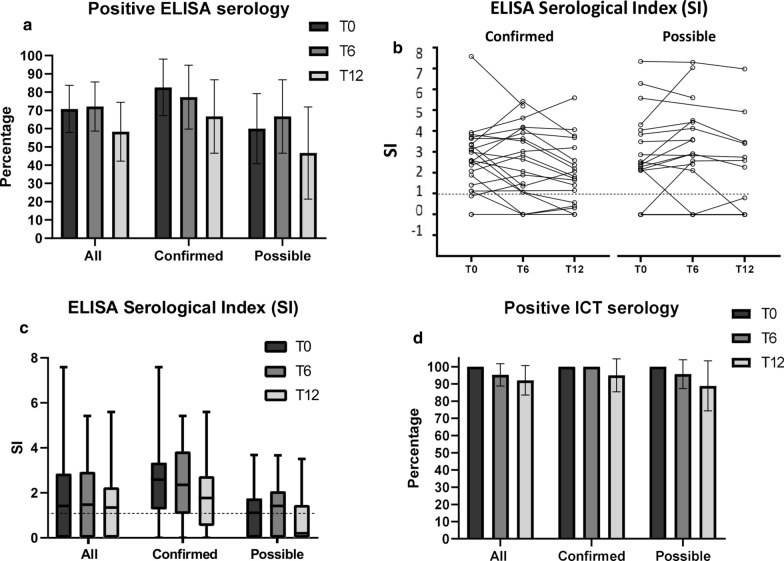
Results: Forty-eight patients were included, 23 confirmed and 25 possible cases. The percentage seropositivity and median antibody titers did not change significantly during follow-up. UCP-LF CAA was positive in 86.9% of confirmed and 20% of possible cases. The percentage positivity and median CAA levels decreased significantly post-treatment, with only two patients having positive CAA levels at T12.
Conclusions: The UCP-LF CAA assay proved useful for the diagnosis of active infection with Schistosoma spp. and highly valuable for post-treatment monitoring in migrants, encouraging the development of a commercial test.
Keywords: Circulating anodic antigen (CAA); Diagnosis; Follow-up; Microscopy; Migrants; Schistosomiasis; Serology.
Conflict of interest statement
All authors declare that they have no conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
