

Robotic Prostatectomy and Prostate Cancer-Related Medicaid Spending: Evidence from New York State
- PMID: 33751413
- PMCID: PMC8606383
- DOI: 10.1007/s11606-021-06680-1
Robotic Prostatectomy and Prostate Cancer-Related Medicaid Spending: Evidence from New York State
Abstract
Background: Robotic prostatectomy is a costly new technology, but the costs may be offset by changes in treatment patterns. The net effect of this technology on Medicaid spending has not been assessed.
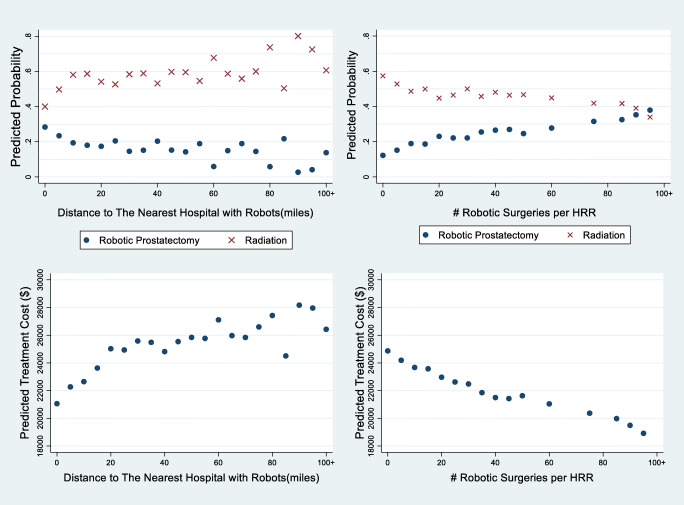
Objective: To identify the association of the local availability of robotic surgical technology with choice of initial treatment for prostate cancer and total prostate cancer-related treatment costs.
Design and participants: This cohort study used New York State Medicaid data to examine the experience of 9564 Medicaid beneficiaries 40-64 years old who received a prostate biopsy between 2008 and 2017 and were diagnosed with prostate cancer. The local availability of robotic surgical technology was measured as distance from zip code centroids of patient's residence to the nearest hospital with a robot and the annual number of robotic prostatectomies performed in the Hospital Referral Region.
Main measures: Multivariate linear models were used to relate regional access to robots to the choice of initial therapy and prostate cancer treatment costs during the year after diagnosis.
Key results: The mean age of the sample of 9564 men was 58 years; 30% of the sample were White, 26% were Black, and 22% were Hispanic. Doubling the distance to the nearest hospital with a robot was associated with a reduction in robotic surgery rates of 3.7 percentage points and an increase in the rate of use of radiation therapy of 5.2 percentage points. Increasing the annual number of robotic surgeries performed in a region by 10 was associated with a decrease in the probability of undergoing radiation therapy of 0.6 percentage point and a $434 reduction in total prostate cancer-related costs per Medicaid patient.
Conclusions: A full accounting of the costs of a new technology will depend on when it is used and the payment rate for its use relative to payment rates for substitutes.
Keywords: Medicaid; prostate cancer; robotic prostatectomy; substitution.
© 2021. Society of General Internal Medicine.
Conflict of interest statement
The authors declare that they do not have a conflict of interest.
Figures
References
-
- Cutler D, Deaton A, Lleras-Muney A. The determinants of mortality. J Econ Perspect. 2006;20:97–120. doi: 10.1257/jep.20.3.97. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
