

Temporary hospitals in times of the COVID pandemic. An example and a practical view
- PMID: 33752321
- PMCID: PMC8329569
- DOI: 10.37201/req/041.2021
Temporary hospitals in times of the COVID pandemic. An example and a practical view
Abstract
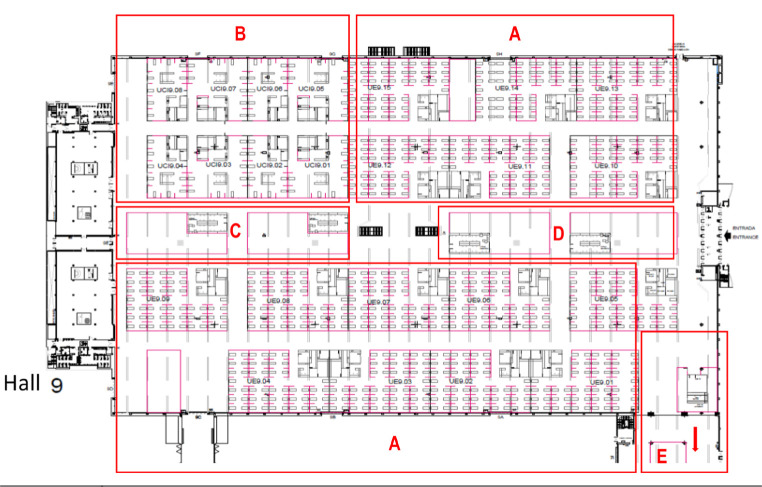
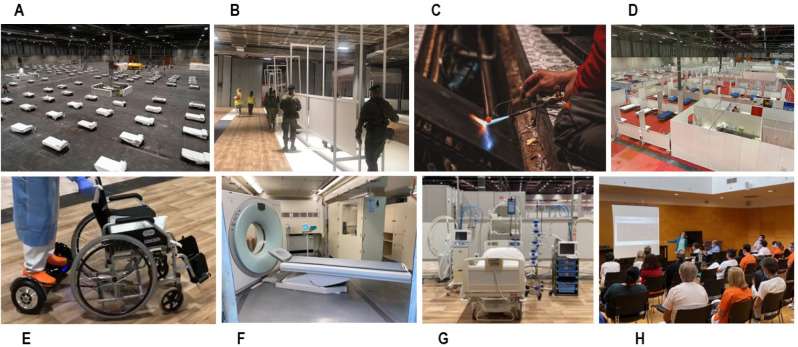
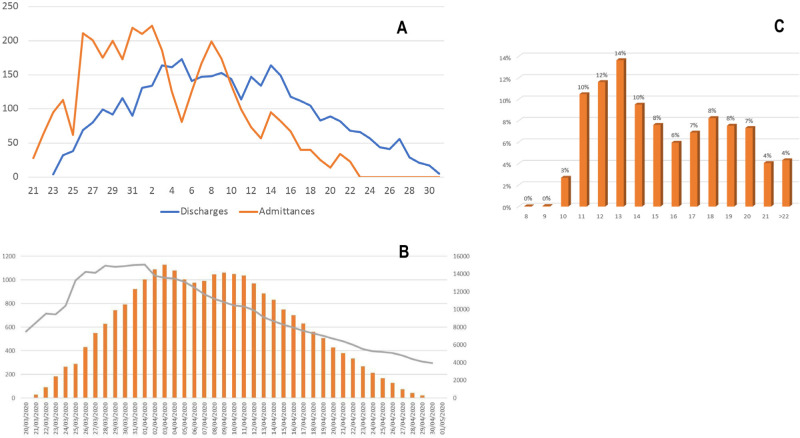
We describe the most widely used temporary hospital in Europe during the first pandemic wave, its structure, function, and achievements. Other models of care developed during the pandemic around the world were reviewed including their capacity, total bed/ICU bed ratio and time of use. We particularly analyzed the common and differential characteristics of this type of facilities. IFEMA Exhibition Center was transformed into a temporary 1,300-bed hospital, which was in continuous operation for 42 days. A total of 3,817 people were treated, generally patients with mild to moderate COVID-19, 91% of whom had pneumonia. The average length of stay was 5 to 36 days. The most frequent comorbidities were hypertension (16.5%), diabetes mellitus (9.1%), COPD (6%), asthma (4.6%), obesity (2.9%) and dementia (1.6%). A total of 113 patients (3%) were transferred to another centers for aggravation, 19 (0.5%) were admitted to ICU and 16 patients (0.4%) died. An element of great help to reducing the overload of care in large hospitals during peaks of health emergencies could be these flexible structures capable of absorbing the excess of patients. These must be safe, breaking domestic transmission and guarantee social and emotional needs of patients. The success of these structures depends on delimitation in admission criteria taking into account the proportion of patients who may require, during admission, assistance in the critical care area.
Describimos el hospital temporal más utilizado en Europa durante la primera ola de la pandemia, su estructura, función y resultados, así como otros modelos de atención desarrollados durante la pandemia en todo el mundo. Se revisa su capacidad, ratio de camas totales/UCI y tiempo de uso. También se describen las características comunes y diferenciales de este tipo de instalaciones. El recinto ferial de IFEMA se convirtió en un hospital temporal de 1.300 camas, que estuvo en funcionamiento continuo durante 42 días. Se atendió a un total de 3.817 personas, en general pacientes con COVID-19 leve a moderada, de los cuales el 91% tenía neumonía. La duración media de la estancia fue de 5 a 36 días. Las comorbilidades más frecuentes fueron la hipertensión (16,5%), la diabetes mellitus (9,1%), la EPOC (6%), el asma (4,6%), la obesidad (2,9%) y la demencia (1,6%). Un total de 113 pacientes (3%) fueron trasladados a otros centros por agravamiento, 19 (0,5%) fueron ingresados en la UCI y 16 pacientes (0,4%) fallecieron. 1200 camas totales con un 8% de camas críticas podría ser una proporción óptima, pero delimitando los criterios de ingreso. La clave para reducir la sobrecarga asistencial en los grandes hospitales durante los picos de emergencias sanitarias reside en estas estructuras flexibles capaces de absorber el exceso de pacientes. Estas deben ser seguras, romper la transmisión doméstica y garantizar las necesidades de atención social y emocional de los pacientes. El éxito de estas estructuras depende de la delimitación en los criterios de admisión teniendo en cuenta la proporción de pacientes que pueden requerir, durante el ingreso, asistencia en el área de cuidados críticos..
Keywords: COVID-19; ICU beds; admission criteria; emergence facilities; emporary hospital; hospital design.
©The Author 2021. Published by Sociedad Española de Quimioterapia. This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International (CC BY-NC 4.0)(https://creativecommons.org/licenses/by-nc/4.0/).
Conflict of interest statement
All authors declare they have no conflicts of interest.
Figures
References
-
- Coronavirus disease (COVID-19) Situation in numbers (by WHO Region) [Internet]. 2021. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019
-
- Spain Becomes Latest Epicenter of Coronavirus After a Faltering Response - The New York Times [Internet]. [cited 2020 May 4]. Available from: https://www.nytimes.com/2020/03/13/world/europe/spain-coronavirus-emerge...
-
- Observatorio de Resultados. Séptimo Informe de Hospitales, 2016- 2018. Available from: http://www.madrid.org/bvirtual/BVCM020357.pdf
-
- Martín MC, León C, Cuñat J, del Nogal F. Recursos estructurales de los Servicios de Medicina Intensiva en España. Med Intensiva. 2013;37(7):443–51. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
