

Outcome of children with oligoarticular juvenile idiopathic arthritis compared to polyarthritis on methotrexate- data of the German BIKER registry
- PMID: 33752685
- PMCID: PMC7986501
- DOI: 10.1186/s12969-021-00522-4
Outcome of children with oligoarticular juvenile idiopathic arthritis compared to polyarthritis on methotrexate- data of the German BIKER registry
Abstract
Background: Oligoarticular juvenile idiopathic arthritis (oligoJIA) is the most commonly diagnosed category of chronic arthritis in children. Nevertheless, there are no evidence- based guidelines for its treatment, in particular for the use of methotrexate (MTX). The primary objective of this analysis is to evaluate the outcomes in patients with persistent oligoJIA compared to those with extended oligoJIA and rheumatoid factor (RF) negative polyarthritis treated with methotrexate.
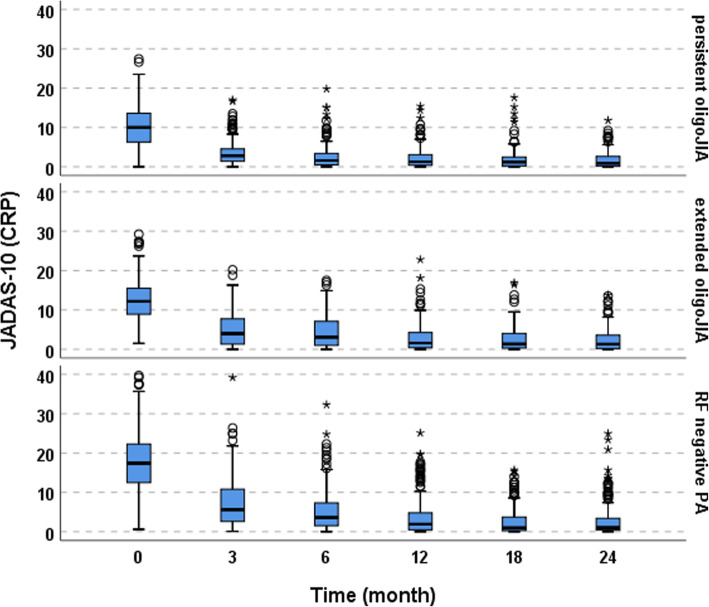
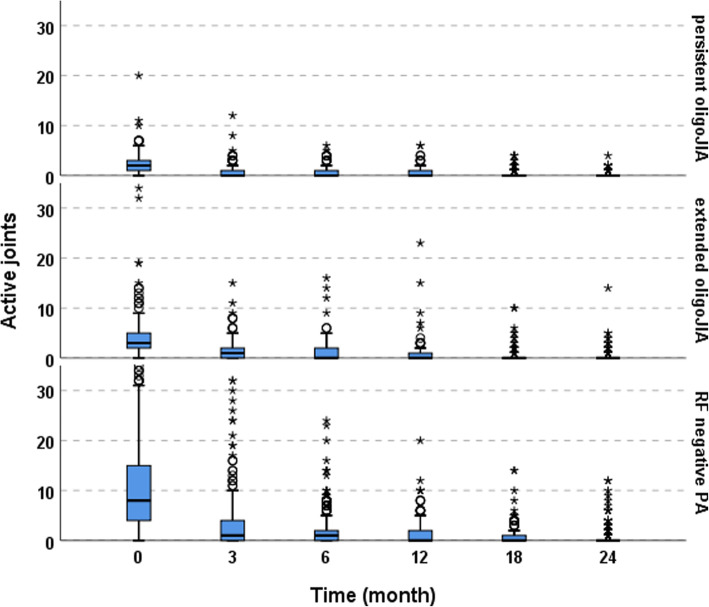
Methods: Patients with persistent or extended oligoJIA or RF negative PA recorded in the Biologics in Pediatric Rheumatology Registry (BiKeR), receiving methotrexate for the first time were included in the analyses. Efficacy was determined using the Juvenile Arthritis Disease Activity Score 10 (JADAS 10). Safety assessment included the documentation of adverse and serious adverse events.
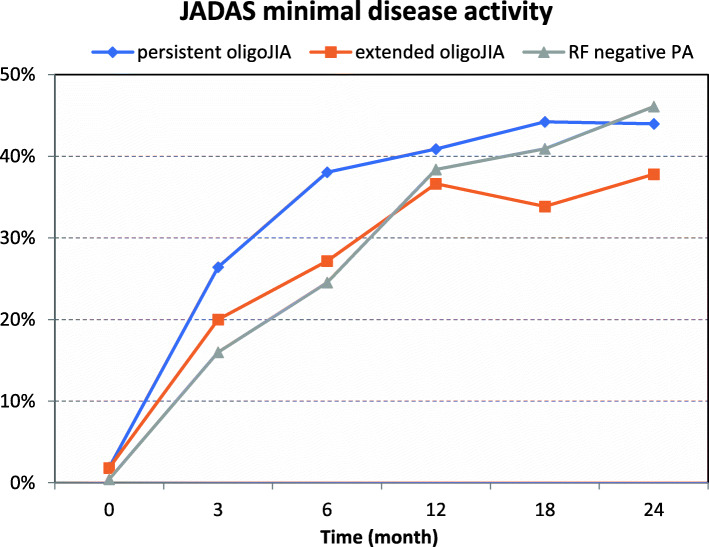
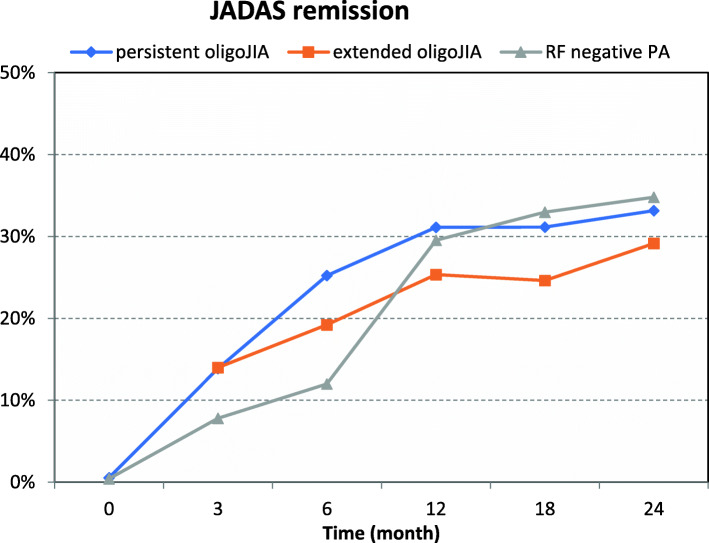
Results: From 2005 through 2011, 1056 patients were included: 370 patients with persistent oligoJIA, 221 patients with extended oligoJIA and 467 patients with RF negative PA. Therapeutic efficacy was observed following the start of methotrexate. Over a period of 24 months JADAS-minimal disease activity (JADAS ≤2) was reached in 44% of patients with persistent oligoJIA, 38% with extended oligoJIA, 46% with RF negative PA, JADAS-remission defined as JADAS ≤1 was reached in 33% of patients with persistent oligoJIA, 29% with extended oligoJIA and 35% (RF negative PA). Patients with extended oligoJIA achieved JADAS remission significantly later and received additional biologic disease-modifying drugs significantly more often than patients with persistent oligoJIA or RF negative PA (p < 0.001). Tolerability was comparable. New onset uveitis occurred in 0.3 to 2.2 per 100 patient years.
Conclusions: Patients with persistent oligoJIA taking methotrexate are at least as likely to enter remission as patients with extended oligo JIA or polyarticular JIA. Patients with extended oligoJIA achieved JADAS remission significantly later. Within 2 years, almost half of the patients with persistent oligoJIA achieved JADAS-minimal disease activity.
Keywords: Comparison; Methotrexate; Oligoarticular juvenile idiopathic arthritis; Outcome; Polyarthritis.
Conflict of interest statement
AR has no conflict of interest. AK has received congress travel fees from Sobi, Sandoz and advisory board honoraria from Celgene. DH has no conflict of interest. FD has received speaker’s fees from Abbvie, Novartis and Pfizer. FWH: has no conflict of interest in regard to this study.GH has received unrestricted funding from Abbvie, Chugai, MSS, Pfizer, Novartis and Roche and personal fees from Bayer, Sobi, Novartis and Pfizer. IF participated on: advisory boards BMS, Amgen, Novartis, Chugai, Abbvie and Pfizer. JKD has no conflict of interest in regard to this study. TK has no conflict of interest in regard to this study.
Figures
References
-
- Petty RE, Southwood TR, Manners P, Baum J, Glass DN, Goldenberg J, et al. International League of Associations for Rheumatology classification of juvenile idiopathic arthritis: second revision, Edmonton, 2001. J Rheumatol. 2004;31(2):390–392. - PubMed
-
- Martini A, Ravelli A, Avcin T, Beresford MW, Burgos-Vargas R, Cuttica R, et al. Toward New Classification Criteria for Juvenile Idiopathic Arthritis: First Steps, Pediatric Rheumatology International Trials Organization International Consensus. J Rheumatol. 2019;46(2):190–197. doi: 10.3899/jrheum.180168. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
