

Cardiovascular magnetic resonance accurately detects obstructive coronary artery disease in suspected non-ST elevation myocardial infarction: a sub-analysis of the CARMENTA Trial
- PMID: 33752696
- PMCID: PMC7983380
- DOI: 10.1186/s12968-021-00723-6
Cardiovascular magnetic resonance accurately detects obstructive coronary artery disease in suspected non-ST elevation myocardial infarction: a sub-analysis of the CARMENTA Trial
Abstract
Background: Invasive coronary angiography (ICA) is still the reference test in suspected non-ST elevation myocardial infarction (NSTEMI), although a substantial number of patients do not have obstructive coronary artery disease (CAD). Early cardiovascular magnetic resonance (CMR) may be a useful gatekeeper for ICA in this setting. The main objective was to investigate the accuracy of CMR to detect obstructive CAD in NSTEMI.
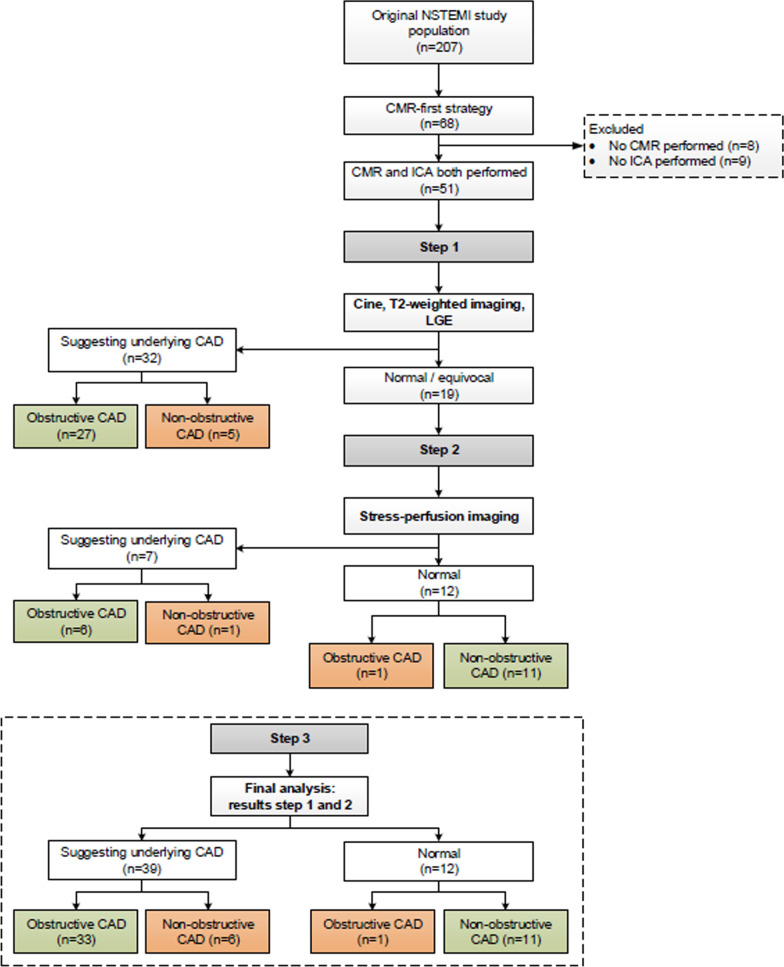
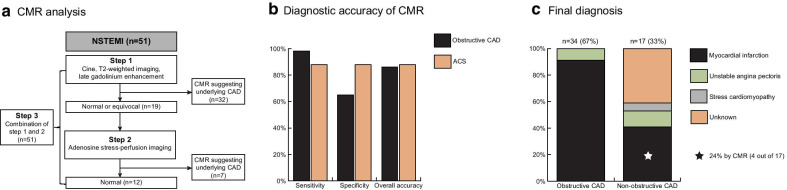
Methods: This study is a sub-analysis of a randomized controlled trial investigating whether a non-invasive imaging-first strategy safely reduced the number of ICA compared to routine clinical care in suspected NSTEMI (acute chest pain, non-diagnostic electrocardiogram, high sensitivity troponin T > 14 ng/L), and included 51 patients who underwent CMR prior to ICA. A stepwise approach was used to assess the diagnostic accuracy of CMR to detect (1) obstructive CAD (diameter stenosis ≥ 70% by ICA) and (2) an adjudicated final diagnosis of acute coronary syndrome (ACS). First, in all patients the combination of cine, T2-weighted and late gadolinium enhancement (LGE) imaging was evaluated for the presence of abnormalities consistent with a coronary etiology in any sequence. Hereafter and only when the scan was normal or equivocal, adenosine stress-perfusion CMR was added.
Results: Of 51 patients included (63 ± 10 years, 51% male), 34 (67%) had obstructive CAD by ICA. The sensitivity, specificity and overall accuracy of the first step to diagnose obstructive CAD were 79%, 71% and 77%, respectively. Additional vasodilator stress-perfusion CMR was performed in 19 patients and combined with step one resulted in an overall sensitivity of 97%, specificity of 65% and accuracy of 86%. Of the remaining 17 patients with non-obstructive CAD, 4 (24%) had evidence for a myocardial infarction on LGE, explaining the modest specificity. The sensitivity, specificity and overall accuracy to diagnose ACS (n = 43) were 88%, 88% and 88%, respectively.
Conclusion: CMR accurately detects obstructive CAD and ACS in suspected NSTEMI. Non-obstructive CAD is common with CMR still identifying an infarction in almost one-quarter of patients. CMR should be considered as an early diagnostic approach in suspected NSTEMI.
Trial registration: The CARMENTA trial has been registered at ClinicalTrials.gov with identifier NCT01559467.
Keywords: Acute coronary syndrome; Cardiovascular magnetic resonance; Coronary angiography; Coronary artery disease; Diagnostic accuracy; High-sensitivity cardiac troponin; Non-ST elevation myocardial infarction.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Nestelberger T, Wildi K, Boeddinghaus J, Twerenbold R, Reichlin T, Gimenez MR, et al. Characterization of the observe zone of the ESC 2015 high-sensitivity cardiac troponin 0h/1h-algorithm for the early diagnosis of acute myocardial infarction. Int J Cardiol. 2016;207:238–245. doi: 10.1016/j.ijcard.2016.01.112. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
