

Comparison of clinical outcomes between nurse practitioner and registrar-led medical emergency teams: a propensity-matched analysis
- PMID: 33752731
- PMCID: PMC7986296
- DOI: 10.1186/s13054-021-03534-4
Comparison of clinical outcomes between nurse practitioner and registrar-led medical emergency teams: a propensity-matched analysis
Abstract
Objective: Medical emergency teams (MET) are mostly led by physicians. Some hospitals are currently using nurse practitioners (NP) to lead MET calls. These are no studies comparing clinical outcomes between these two care models. To determine whether NP-led MET calls are associated with lower risk of acute patient deterioration, when compared to intensive care (ICU) registrar (ICUR)-led MET calls.
Methods: The composite primary outcome included recurrence of MET call, occurrence of code blue or ICU admission within 24 h. Secondary outcomes were mortality within 24 h of MET call, length of hospital stay, hospital mortality and proportion of patients discharged home. Propensity score matching was used to reduce selection bias from confounding factors between the ICUR and NP group.
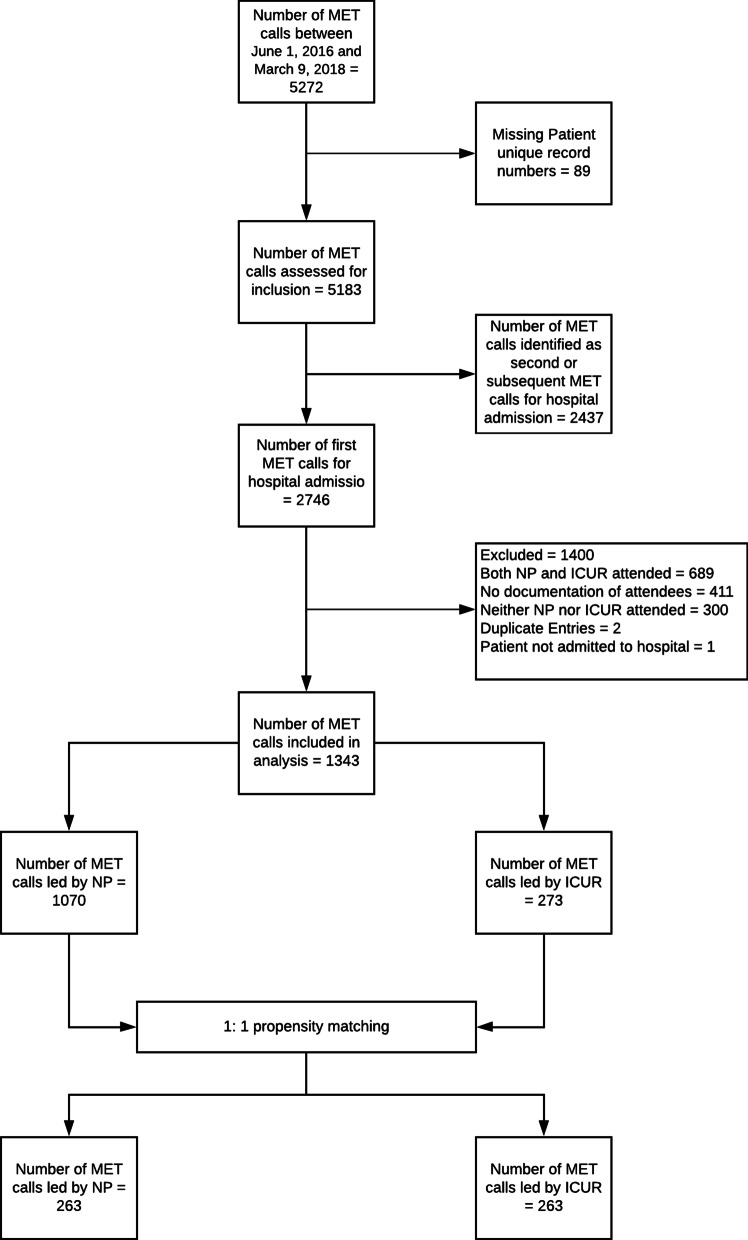
Results: A total of 1343 MET calls were included (1070 NP, 273 ICUR led). On Univariable analysis, the incidence of the primary outcome was higher in ICUR-led MET calls (26.7% vs. 20.6%, p = 0.03). Of the secondary outcome measures, mortality within 24 h (3.4% vs. 7.7%, p = 0.002) and hospital mortality (12.7% vs. 20.5%, p = 0.001) were higher in ICUR-led MET calls. Propensity score-matched analysis of 263 pairs revealed the composite primary outcome was comparable between both groups, but NP-led group was associated with reduced risk of hospital mortality (OR 0.57, 95% CI 0.35-0.91, p = 0.02) and higher likelihood of discharge home (OR 1.55, 95% CI 1.09-2.2, p = 0.015).
Conclusion: Acute patient deterioration was comparable between ICUR- and NP-led MET calls. NP-led MET calls were associated with lower hospital mortality and higher likelihood of discharge home.
Keywords: Deterioration; Discharge; Medical emergency team; Mortality.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Mitchell OJL, Motschwiller CW, Horowitz JM, Evans LE, Mukherjee V. Characterising variation in composition and activation criteria of rapid response and cardiac arrest teams: a survey of Medicare participating hospitals in five American states. BMJ Open. 2019;9(3):e024548. doi: 10.1136/bmjopen-2018-024548. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
