

Exercise right ventricular ejection fraction predicts right ventricular contractile reserve
- PMID: 33752973
- PMCID: PMC8169559
- DOI: 10.1016/j.healun.2021.02.005
Exercise right ventricular ejection fraction predicts right ventricular contractile reserve
Abstract
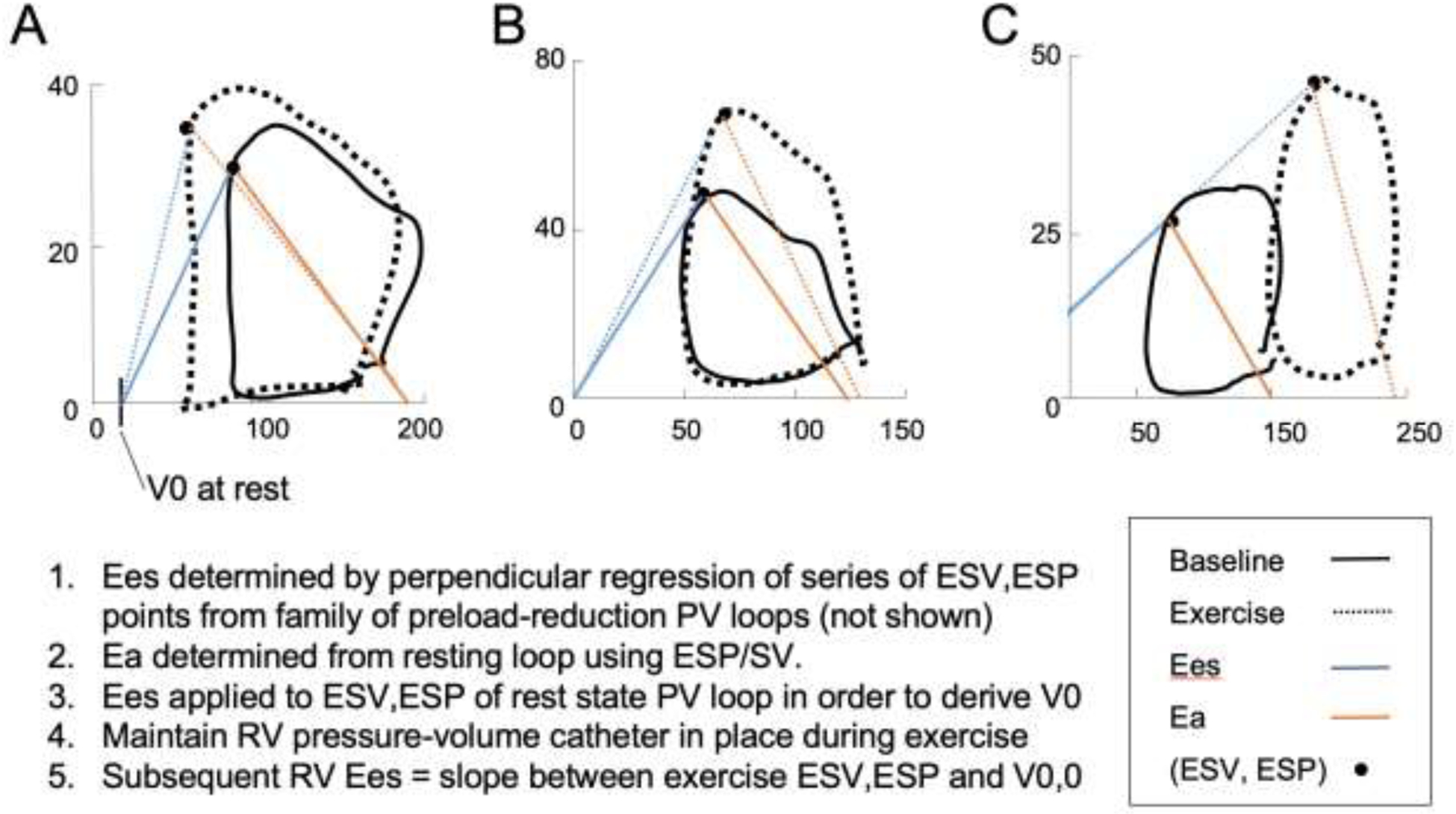
Background: Right ventricular (RV) contractile reserve shows promise as an indicator of occult RV dysfunction in pulmonary vascular disease. We investigated which measure of RV contractile reserve during exercise best predicts occult RV dysfunction and clinical outcomes.
Methods: We prospectively studied RV contractile reserve in 35 human subjects referred for right heart catheterization for known or suspected pulmonary hypertension. All underwent cardiac magnetic resonance imaging, echocardiography, and supine invasive cardiopulmonary exercise testing with concomitant RV pressure-volume catheterization. Event-free survival was prospectively adjudicated from time of right heart catheterization for a 4-year follow-up period.
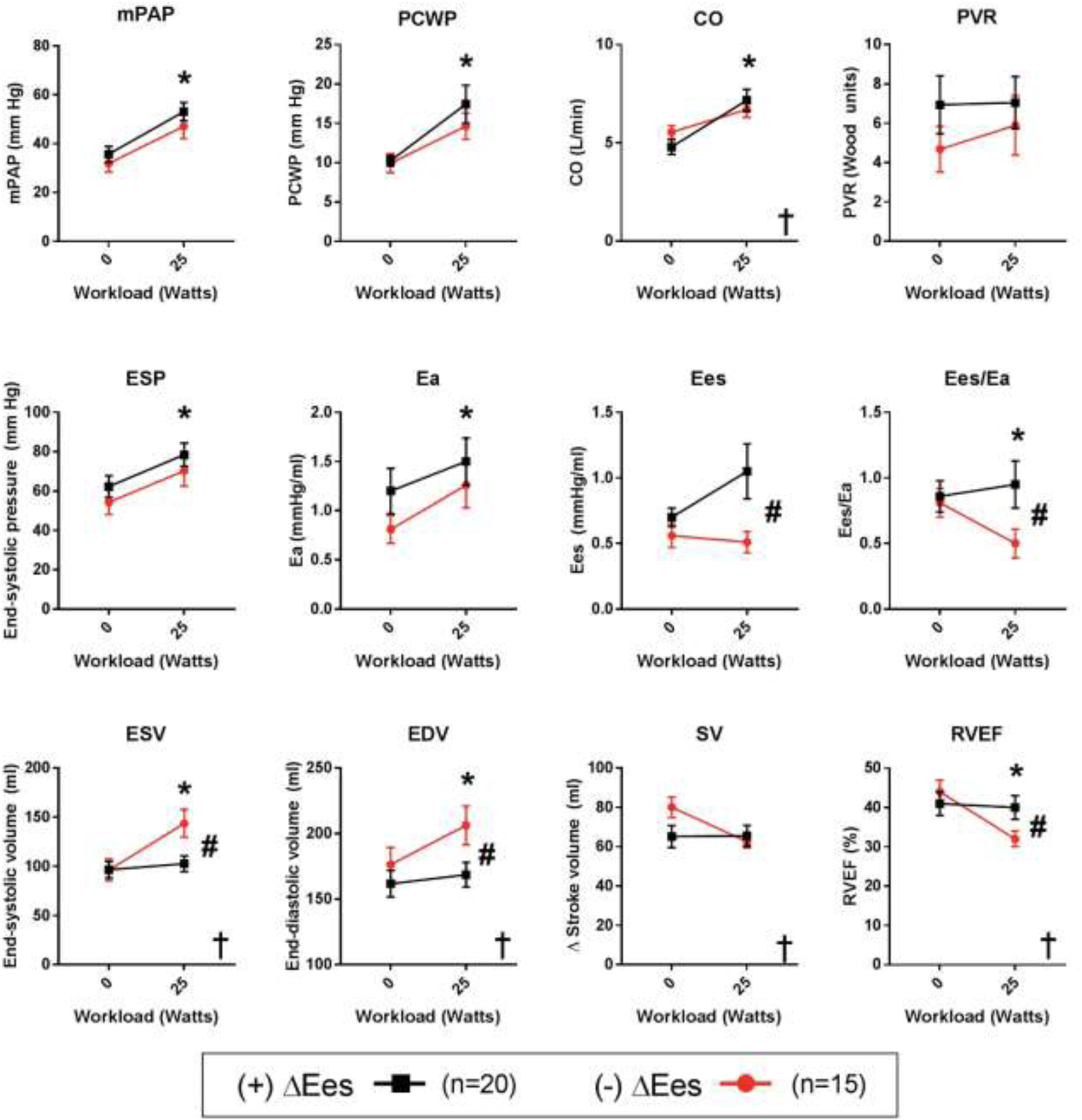
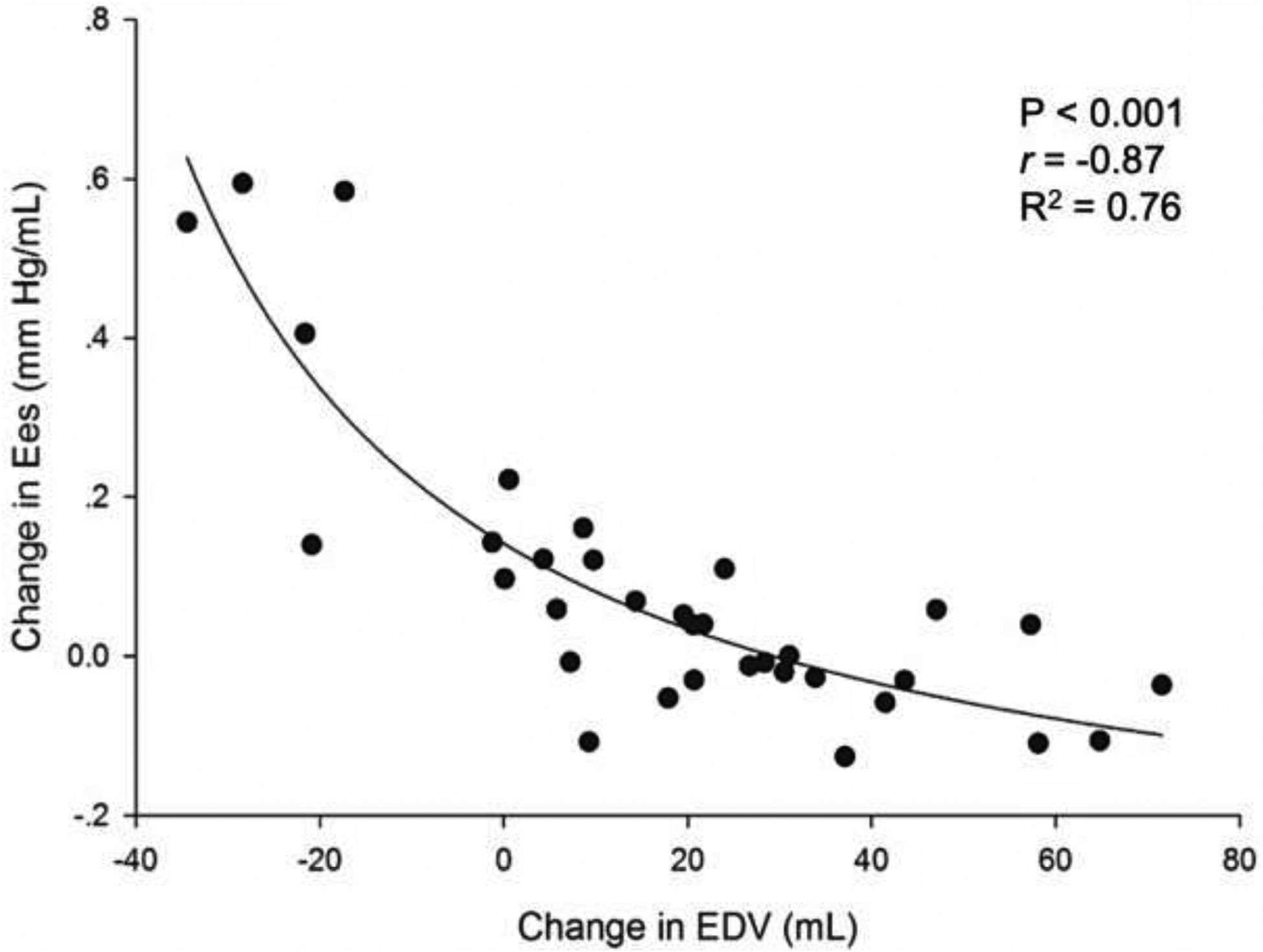
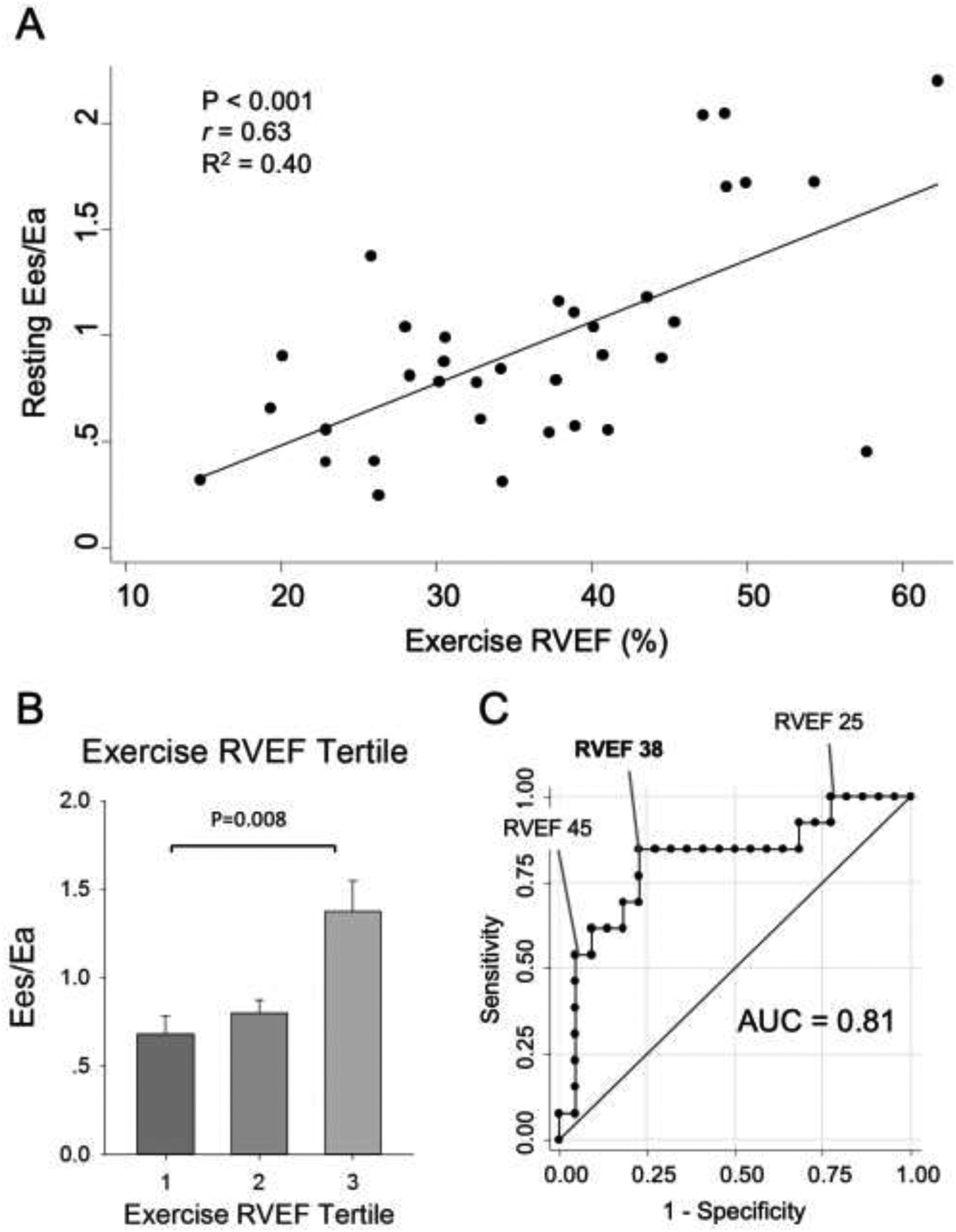
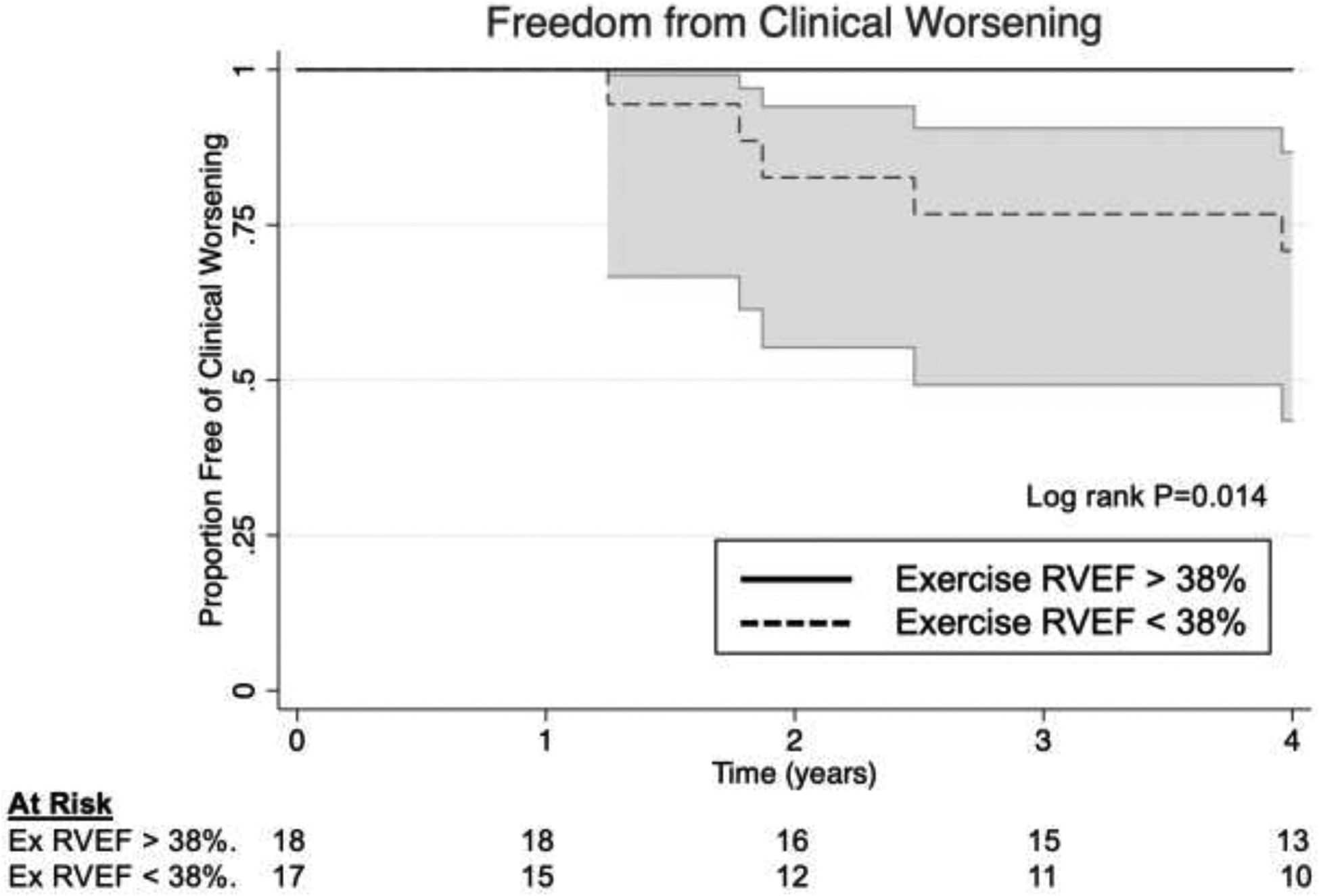
Results: RV contractile reserve during exercise, as measured by a positive change in end-systolic elastance (Ees) during exertion, was associated with elevation in pulmonary pressures but preservation of RV volumes. Lack of RV reserve, on the other hand, was tightly coupled with acute RV dilation during exertion (R2 = 0.76, p< 0.001). RV Ees and dilation changes each predicted resting RV-PA dysfunction. RV ejection fraction during exercise, which captured exertional changes in both RV Ees and RV dilation, proved to be a robust surrogate for RV contractile reserve. Reduced exercise RV ejection fraction best predicted occult RV dysfunction among a variety of resting and exercise RV measures, and was also associated with clinical worsening.
Conclusions: RV ejection fraction during exercise, as an index of RV contractile reserve, allows for excellent identification of occult RV dysfunction, more so than resting measures of RV function, and may predict clinical outcomes as well.
Keywords: exercise; heart ventricles; pulmonary hypertension.
Copyright © 2021 International Society for Heart and Lung Transplantation. Published by Elsevier Inc. All rights reserved.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
