

Simple Sugar and Sugar-Sweetened Beverage Intake During Adolescence and Risk of Colorectal Cancer Precursors
- PMID: 33753105
- PMCID: PMC8238879
- DOI: 10.1053/j.gastro.2021.03.028
Simple Sugar and Sugar-Sweetened Beverage Intake During Adolescence and Risk of Colorectal Cancer Precursors
Abstract
Background & aims: Recent increasing trends in early-onset colorectal cancer (CRC) strongly supports that early-life diet is involved in CRC development. However, data are lacking on the relationship with high sugar intake during early life.
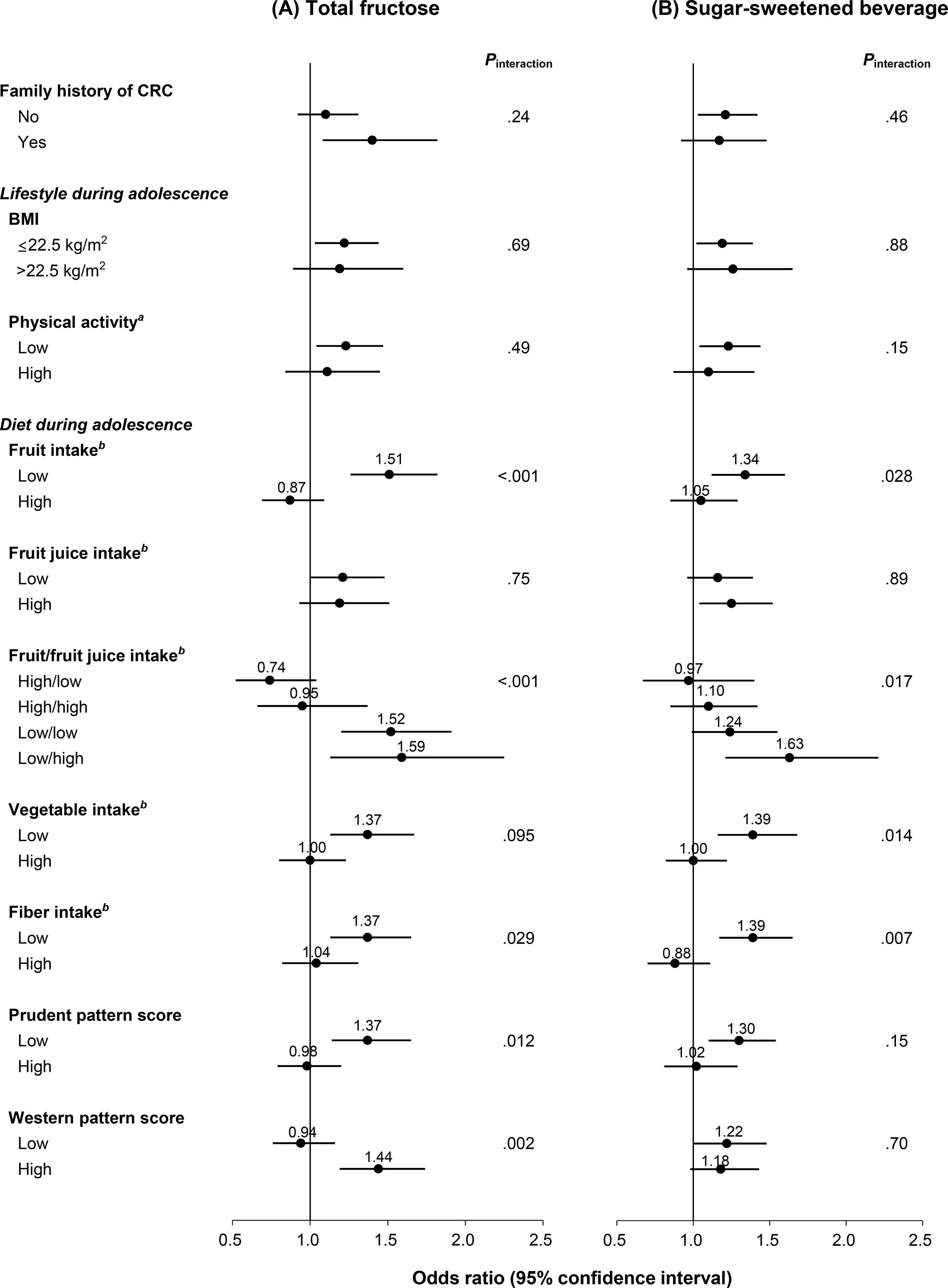
Methods: We prospectively investigated the association of adolescent simple sugar (fructose, glucose, added sugar, total sugar) and sugar-sweetened beverage (SSB) intake with CRC precursor risk in 33,106 participants of the Nurses' Health Study II who provided adolescent dietary information in 1998 and subsequently underwent lower gastrointestinal endoscopy between 1999 and 2015. Odds ratios (ORs) and 95% confidence intervals (CIs) were estimated using logistic regression for clustered data.
Results: During follow-up, 2909 conventional adenomas (758 high-risk) and 2355 serrated lesions were identified (mean age at diagnoses, 52.2 ± 4.3 years). High sugar and SSB intake during adolescence was positively associated with risk of adenoma, but not serrated lesions. Per each increment of 5% of calories from total fructose intake, multivariable ORs were 1.17 (95% CI, 1.05-1.31) for total and 1.30 (95% CI, 1.06-1.60) for high-risk adenoma. By subsite, ORs were 1.12 (95% CI, 0.96-1.30) for proximal, 1.24 (95% CI, 1.05-1.47) for distal, and 1.43 (95% CI, 1.10-1.86) for rectal adenoma. Per 1 serving/day increment in SSB intake, ORs were 1.11 (95% CI, 1.02-1.20) for total and 1.30 (95% CI, 1.08-1.55) for rectal adenoma. Contrary to adolescent intake, sugar and SSB intake during adulthood was not associated with adenoma risk.
Conclusions: High intake of simple sugars and SSBs during adolescence was associated with increased risk of conventional adenoma, especially rectal adenoma.
Keywords: Cancer Epidemiology; Colorectal Adenoma; Colorectal Polyp; Conventional Adenoma; Fructose.
Copyright © 2021 AGA Institute. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Sugary Truth of Early-Onset Colorectal Neoplasia-Not So Sweet After All.Gastroenterology. 2021 Jul;161(1):27-29. doi: 10.1053/j.gastro.2021.04.046. Epub 2021 Apr 24. Gastroenterology. 2021. PMID: 33905675 No abstract available.
-
PAVK: Ein bisschen Training ist zu wenig.MMW Fortschr Med. 2021 Jul;163(13):10. doi: 10.1007/s15006-021-0032-3. MMW Fortschr Med. 2021. PMID: 34240349 German. No abstract available.
-
Zuckerkonsum in der Jugend erhöht späteres Darmkrebsrisiko.MMW Fortschr Med. 2021 Jul;163(13):10. doi: 10.1007/s15006-021-0168-1. MMW Fortschr Med. 2021. PMID: 34240350 German. No abstract available.
References
-
- Arnold M, Sierra MS, Laversanne M, et al. Global patterns and trends in colorectal cancer incidence and mortality. Gut 2017;66:683–691. - PubMed
-
- Siegel RL, Jakubowski CD, Fedewa SA, et al. Colorectal Cancer in the Young: Epidemiology, Prevention, Management. Am Soc Clin Oncol Educ Book 2020;40:1–14. - PubMed
-
- Keum N, Giovannucci E. Global burden of colorectal cancer: emerging trends, risk factors and prevention strategies. Nat Rev Gastroenterol Hepatol 2019;16:713–732. - PubMed
-
- Siegel RL, Miller KD, Goding Sauer A, et al. Colorectal cancer statistics, 2020. CA Cancer J Clin 2020;70:145–164. - PubMed
-
- SEER Cancer Stat Facts: CRC National Cancer Institute. Bethesda, MD. Available at seer.cancer.gov/statfacts/html/colorect.html
Publication types
MeSH terms
Substances
Grants and funding
- R35 CA197735/CA/NCI NIH HHS/United States
- U01 HL145386/HL/NHLBI NIH HHS/United States
- R21 CA230873/CA/NCI NIH HHS/United States
- R01 CA067262/CA/NCI NIH HHS/United States
- K24 DK098311/DK/NIDDK NIH HHS/United States
- R01 CA205406/CA/NCI NIH HHS/United States
- R03 CA197879/CA/NCI NIH HHS/United States
- R35 CA253185/CA/NCI NIH HHS/United States
- R21 CA222940/CA/NCI NIH HHS/United States
- R01 CA151993/CA/NCI NIH HHS/United States
- U01 CA176726/CA/NCI NIH HHS/United States
- K07 CA188126/CA/NCI NIH HHS/United States
- R33 CA160344/CA/NCI NIH HHS/United States
- K99 CA215314/CA/NCI NIH HHS/United States
- R00 CA215314/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
